The application of systems theory
| ✅ Paper Type: Free Essay | ✅ Subject: Social Work |
| ✅ Wordcount: 4669 words | ✅ Published: 07 Mar 2017 |
The Application Of Systems Theory
To a Case Study
Introduction
The following case study will detail an intervention with a 32-year old service user who was referred with a range of presenting issues and needs. It was apparent that a complex array of family, social and agency networks existed, indicating that the focus of any intervention would necessitate the addressing of these various components and their role in the service user’s functioning. It was decided that employing systems theory would be the most efficacious approach in managing the service user’s needs.
General systems theory was first proposed by von Bertalanffy (1968) as a universal theory of the organisation of parts into wholes. A system was defined as “a complex of interacting elements”. Although this paradigm was initially applied to the physical world (mathematics, biochemistry, etc), it was adopted by the therapeutic community in order to formulate an understanding of systems comprising individuals and organisations. Some of the ideas and concepts systems theory has brought to the field include:
- Families and other social groups are systems having properties which are more than the sum of the properties of their parts.
- Every system has a boundary, the properties of which are important in understanding how the system works.
- Changes within systems can occur, or be stimulated, in various ways.
- Communication and feedback mechanisms between the parts of a system are important in the functioning of the system.
- Events such as the behaviour of individuals in a family are better understood as examples of circular causality, rather than as being based on linear causality.
- Systems are made up of subsystems (e.g. parental, marital, siblings) which are themselves parts of larger suprasystems (e.g. extended family, the neighbourhood, hospital).
(Beckett, 1973).
The service user was a 32-year old male of Afro-Caribbean origins, with a diagnosis of schizoaffective disorder dating back to his early teens. He had been residing in a semi-secure forensic unit for more than two years and was detained under Section 3 of the Mental Health Act. In terms of family history, he had been conceived through rape and fostered by distant relatives in Trinidad. Upon the death of his foster mother, his natural mother arranged for him to leave Trinidad and enter the UK. Shortly after this, he became involved with the mental health system and the criminal justice system. Subsequently, his mother had refused all contact with him and would not engage with any of his care. The sole family contact had been his maternal grandmother.
A genogram is a useful adjunct within assessment and treatment when utilising systems theory (e.g. Guerin and Pendagast, 1976), in that it gives a concise graphic summary of the composition of the systems surrounding an individual. A genogram depicting DE’s particular systems was prepared and is illustrated in Figure 1.
Within the genogram, DE’s familial relationships are illustrated, showing the existing subsystem with his maternal grandmother. Other subsystems include, DE’s relationships with the criminal justice system, mental health services and with myself, his social worker.
With regard to using systems theory in my assessment and intervention of DE, this would encompass developing a hypothesis concerning the nature of the relationships DE has with aspects of his system and how this impacts upon his functioning. In addition, circular questioning would be employed to test this hypothesis and promote change (e.g. Selvini Palazzoli, Cechin, Prata and Boscolo, 1980a). Each of DE’s presenting needs will be explored within the context of his wider system and the methodology inherent to systems theory employed in my intervention.
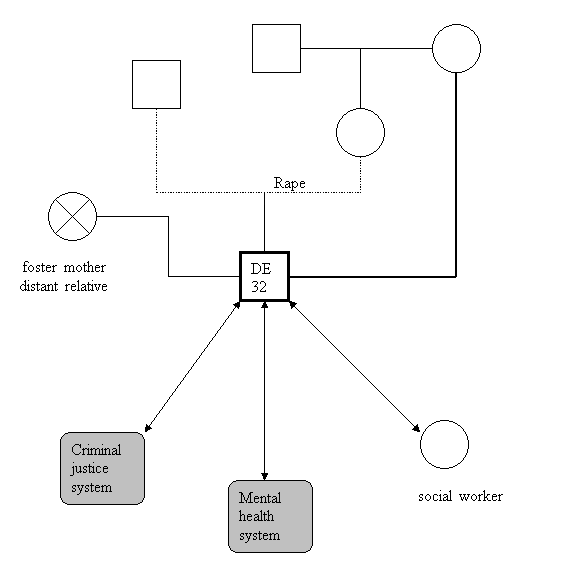
Figure 1: A genogram of DE’s case.
The Referral
DE was a statutory referral which was accompanied by a challenge from his legal representatives to the local authority, claiming that they had failed in their duties towards DE as he was medically fit for discharge and did not need to be detained under Section 3 of the Mental Health Act. Although discharge from Section 3 was agreed, no plans were presented to the mental health tribunal by the local authority regarding the arrangement of appropriate accommodation. From the perspective of the social worker, plans were therefore required to implement Section 117 and organise appropriate after care and accommodation. In order to do this, it was necessary to identify DE’s wishes and preferences as far as possible, in addition to managing any risk perceived by the multidisciplinary team and the mental health tribunal. A transfer CPA to the community team was organised in order to maintain DE in the community and facilitate his recovery. Adhering to the notion of “goodness of fit”, inherent to systems theory (Payne, 2002), that is enhancing the match between the individual and their environment, ways of developing, maintaining or strengthening supportive interventions and reducing, challenging or replacing stressful systems were explored.
Assessment
An assessment of DE’s presenting needs was conducted in order to formulate a hypothesis based upon the information available which would then provide a starting point and guide to subsequent interventions. According to Selvini Palazzoli et al. (1980a), a hypothesis is “neither true, nor false, but more or less useful”. Therefore, it was important to maintain this stance when considering the circumstances surrounding DE’s case. By seeking information from DE and others within his system, I was able to obtain as many perspectives as possible and construct an understanding, or story, as to how he had come to be “stuck” and enable him to move in a more helpful direction.
Both DE and the multidisciplinary team involved in his care agreed that he required 24 hour residential care, as previous supported accommodation had not been able to facilitate his needs and he had relapsed, leading to his admission to hospital under section. Additional presenting concerns reported by DE included an impoverished family support network and poor finances. Drug and alcohol misuse were also evident, acknowledged by DE and verified by a positive test for cocaine. DE’s keyworker recounted how DE frequently disengaged with him and displayed challenging behaviour, including breaking rules of the care home and absconding. Indicators of relapse described by staff included a preoccupation with insect infestation, delusions of the devil attacking him and homophobic fears of male staff sexually assaulting him. In addition, non-compliance with his care plan was recognised as a precursor to relapse.
Using circular questions to derive new information about DE’s situation and the interconnectedness of the system’s components, a pattern emerged which suggested possible indicators of relapse. A principal feature of circularity is the capacity of the therapist to consider feedback from the systems involved and to invite each part of the system to relate their perspectives of other subsystems, thereby metacommunicating (Selvini Palazzoli et al. 1980a; Byng-Hall, 1988; Cecchin, 1987). Further crucial principles of circularity are asking about specific behaviours that occur, rather than feelings or interpretations and ranking behaviours in order to highlight differences (Barker, 1998; Dallos and Draper, 2000). So, for example, DE’s keyworker was asked: “what does DE do when he breaks the rules in the house”, “when you believe DE is relapsing, how do you know? What does he say or do?”, “who is most worried about DE using drugs/alcohol?”. Similarly, DE was asked such questions as: “when you abscond from the care home, who is most concerned? … and then who?”, “when you are worried about the devil attacking you, what do you do?”, “what would your keyworker say was most important for you to get sorted out?”.
A specific use of circular questioning is to define the problem (Bentovim and Bingley Miller, 2002). Hence, members of DE’s system, including his key worker, other multidisciplinary team workers, available family members and DE himself were questioned as to “what is the problem? What do you think DE/keyworker/etc would say is the problem? Who agrees with DE? Who disagrees? Who is it most a problem for?…” etc. Such information served to enrich the hypothesis that was being formulated of DE’s needs.
Over time, a systemic hypothesis evolved which incorporated the role of impaired family functioning and an early sense of abandonment by DE’s natural mother combined with the loss of his secondary, foster mother contributing to the development of a schizoaffective disorder. A further contributing factor may have been DE’s move to the UK following his bereavement and the sense of confusion and alienation this may have instilled. A pre-existing vulnerability to his mental health problems may have been activated by DE’s use of drugs and alcohol, possibly his coping mechanism to manage the previously described stressors.
In terms of DE’s behaviour within his care home, it would be important to consider physiological factors many of the concerns reported. The literature associated with schizoaffective disorders has suggested that the onset of the illness can produce cognitive deficits, including memory impairment, planning, social judgement and insight (Randolph, Goldberg and Weinberger, in Heilman & Valenstein, 1993; James and Murray, 1991). These deficits, combined with the lack of family support and underlying psychological issues, could have resulted in the issues with compliance and rule-breaking reported by the professionals involved in DE’s care.
However, within a systemic approach, it is important to consider the dynamic interplay between the individual and the various components of their system when conceptualising the problem. In DE’s case, it appeared that the effects of his drug and alcohol use and of rejection issues had not been fully considered by staff at the care home and therefore the consequences of these had been able to escalate into relapse. Furthermore, it may have been that an over-critical attitude towards DE prevailed within his care home, as has been described in the concept of expressed emotion (Leff, 1994). This has generally been reported as existing within the families of those with schizoaffective disorders and is thought to represent deficits in communication and overinvolvement.
The function of the problem is also a vital element within a systemic formulation (Reder and Fredman, 1996; Bilson and Ross, 1999) and in DE’s case his presenting issues appeared to represent both a communication of internal conflicts (loss, abandonment, etc) and as a solution to the problem perceived by him as inappropriate accommodation. Thus, his behaviour could be conceptualised as an attempt to resolve both internal and external discordance. However, clearly DE’s perceived solution only served to escalate and maintain the essential difficulty, that of his lack of engagement with help and disruptive behaviour.
Intervention
There were various strands to my intervention with DE, within which I attempted to address the issues outlined in the above hypotheses. Initially, the issue of accommodation was addressed. In concordance with a systemic approach, DE’s needs and preferences, as well as opinions derived from members of the multi-disciplinary team, were matched with available accommodation. Three suitable placements were identified which were concomitant with the needs identified in DE’s care plan, that is: 24 hour residential accommodation with staff to supervise his medication, encourage independent living skills and monitor his activities and behaviour to identify relapse indicators. DE’s opinions on the three potential placements were sought and a decision reached on the most suitable. In view of DE’s history of lack of engagement with keyworkers, it was felt that regular meetings with his care co-ordinator would be vital in exploring his concerns and potential barriers to compliance with his care plan. The use of circular questioning could be usefully extended in such meetings, in reframing DE’s perception of his concerns and enabling him to recognising the effects of his behaviour on himself and others.
Specific aspects of DE’s presenting problems were managed by referral to appropriate agencies, thus widening his system of support. For the substance misuse reported he was referred to a drug and alcohol worker. A referral to psychological services was made to address his rejection and bereavement issues. The involvement of DE’s grandmother and uncle was also an integral part of discussing his difficulties and it was postulated that at some point in the future, systemic family therapy might be helpful in providing some cohesion to DE’s family structure and enabling communication with this part of his system.
Once the initial concerns had been addressed, my role turned towards care management and a reasonable price for the accommodation was negotiated, along with the development of a comprehensive care plan which was presented to the agency’s funding panel. The funding was agreed and a discharge and transfer of care CPA was arranged. Throughout the ensuing discussions of plans, DE’s opinions were sought. In order to best meet the needs identified and ensure an optimal rehabilitation programme, DE’s care plan incorporated day care activities, psychological and community forensic input.
In accordance with the principles of a systems intervention, a non-judgemental stance was maintained throughout (Goldenberg and Goldenberg, 2004) and the notion of partnership was promoted (Dallos and Draper, 2000). Additionally, the strategy of facilitating sustained change whilst not being an expert about the system was adopted (Fleurida, 1986), although this presented certain challenges as will be discussed in the following sections.
In terms of implementing DE’s placement, it was agreed that a gradual transfer which allowed him to adjust to the new setting would ameliorate his opportunities for rehabilitation. Therefore, overnight stays and extended stays for a week prior to discharge were arranged. Initially, difficulties were experienced with DE’s compliance with some house rules and I arranged a meeting with DE and the house manager in order to discuss and negotiate these in order to prevent a breakdown of the placement. Once more, circular questions were used to elucidate the problem and identify possible routes for change. For example, DE was asked, “when you don’t comply with this rule, who is most upset?” and “what prevents you sticking to the rules?”. The house manager was asked questions such as, “What does DE do instead of sticking to the rules?” and “what reasons do you think he has for not complying?”. Consequently, specific barriers and obstacles were identified and it was possible to negotiate a way in which DE could assert his individuality within the placement setting, whilst behaving in ways which were acceptable to staff and other residents. Thus, the “fit” between DE and this particular system was enhanced.
Review and Ending
During my work with DE a dynamic, fluid hypothesis was formed which was based on systemic principles, in that it was circular, addressed relationships, was expressed in terms of what people do and believe rather than what they are and included all members of the system (Reder, 1983). The hypothesis was continually monitored and reframed during the intervention phase, which facilitated change and enabled new perspectives and solutions to be considered.
Other parts of DE’s system were also modified by posing circular questions as they allowed the various professionals and agencies involved to consider how helpful or unhelpful the strategies they employed to manage the exigencies of DE’s case were and to gain different perspectives. It is important to note that this approach is distinct from merely providing instruction or information, in that it facilitates change through the process of thinking and reasoning.
The initial focus of intervention – to provide appropriate accommodation – was successfully completed. This was rendered smoother by the gradual transition to his new setting. By the end of the intervention, I believe that DE was able to engage in a more useful way with the various components of his system and was more settled in his placement as a result. Reports from the house manager and other professionals also indicated that this was the case.
Referrals to other agencies (psychology and drug and alcohol services) which comprised a vital component of the intervention, enabled an expansion of DE’s systems and the meeting of previously unconsidered needs. His progress with these agencies was ongoing. DE’s engagement with community forensic services was valuable in gaining further perspectives into his care.
Discussion
Within systems theory, the questions themselves form a substantial part of the intervention (Tomm, 1988), as they are believed to lead towards a constructive change in the problematic experiences and behaviours of service users. In addition, questions constitute a much stronger invitation for users to become engaged in a conversation and process than do statements, instructions of information and provides stimulation to think through problems alone, thus promoting autonomy and a sense of personal achievement (Payne, 2002).
In continually seeking the views of DE and perspectives from other parts of his system, it was possible to create a clearer picture of the characteristics of the problem and to foster a sense of ownership on the part of DE. That is, because he felt part of the process of change, he would be more likely to feel comfortable with its parameters. A further part of promoting DE’s compliance with his care plan was to use positive connotation, another important principle of systems theory (O’Brian and Bruggen, 1985). Positively connoting DE’s behaviour consisted not only in reinforcing and praising his attempts to change, but also in acknowledging that his problem behaviour was serving to express his dissatisfaction with the situation he was in. An important aspect of intervention therefore was to communicate an understanding of how things had come to be the way they were. Only through doing this was it possible to challenge the existing belief system, suggesting new and different definitions of relationships. Therefore, by acknowledging the pain of DE’s abandonment by his mother with a referral to a psychologist, it enabled him to explore a different way of interacting with this part of his system. Similarly, by considering the role of drugs and alcohol in mediating his distress and enabling him to cope with his situation, other means of coping were explored.
The use of systems theory was congruent with mental health policy guidance for CPA in that it was person focused, involved all relevant agencies and required a recognition of needs in order to facilitate the movement of service users through CPA. The identification of unmet needs in DE’s case, as well as involving multiple agencies was crucial in managing his care effectively. As DE was on enhanced CPA, it was important to consider multiple care needs and to recognise that he was more likely to disengage with care. Once more, a holistic assessment and a comprehensive, multi-disciplinary, multi-agency plan which encapsulated his wider system was necessary.
Systems theory requires strategic thinking about the possibilities and limitations for change in the different systems affecting the user’s environment, as well as an understanding of the possibilities for intervention in each system (deShazer, 1982; Penn, 1982), therefore considering DE’s behaviour in specific settings and with specific individuals and agencies was a useful strategy. In addition, possessing an understanding of the possibilities for intervention within each system enabled me to think creatively about different courses of action and potential outcomes (Byng_Hall, 1988).
Review and Evaluation
In general, systems theory was a useful tool in working with DE, in that its principles guided many aspects of the assessment and intervention towards a beneficial outcome. The basic tenets of systems theory, of being respectful of all perspectives and attempting to empower the service user to implement change, are congruent with the CPA model of working. However, the principle of maintaining neutrality (i.e. forging an alignment with all parts of the system) and a non-judgemental, non expert stance (Selvini Palazzoli et al. 1980a; Fleurida, 1986) proved to be more challenging. As DE’s care co-ordinator it could be expected that a greater alliance would be formed with him and also that I would possess, in this role, information and knowledge pertaining to a variety of issues, such as financial assistance available to him. Clearly in this case, I was unable to maintain a non-expert stance. Furthermore, being non-judgemental in relation to all DE’s presenting needs (for example, his drug and alcohol misuse) was very difficult and whilst my approach could encompass the evolution of a shared understanding of this behaviour, ultimately the negative impact on DE’s mental health and stability of his placement would need to be acknowledged. Therefore, it could be said that there was a juxtaposition between CPA care management and using systems theory. However, it was possible to separate the two aspects of my role with DE and apply systems theory accordingly.
In terms of what I would do differently, I believe that a greater involvement of DE’s family would have been beneficial in order to assist him in constructing a different story or narrative around his history, which would have enriched his and perhaps others’ understanding of why problems were presenting themselves.
Applying systems theory to a service user such as DE, who may have the cognitive deficits previously described, raises some important ethical issues. Firstly, regarding the ability to give consent to such an approach being employed and to the seeking of perspectives from other parts of the system, such as family members and other workers. The potentially harmful influence of labels has been described in the literature of systems theory (e.g. Benson, Long and Sporakowski), however the use of labels such as “schizoaffective” and “enhanced CPA” would seem unavoidable when working within a multidisciplinary team which necessitates communicating with equivalent language. However, the use of systems theory creates space for thinking about the meaning and impact of these labels and is, therefore, at the very least a valuable and functional adjunct to the repertoire of strategies for managing complex cases.
Summary and Conclusion
The work carried out with DE attempted to illustrate how individuals function as a part of many systems – they are affected by these systems and they, in turn, affect the systems. I believe that the circular nature of DE’s presenting issues and needs was highlighted effectively and the intervention took into consideration this dynamic interchange and the consequences that changes in one part of a system will have for other parts. Fundamentally, I have learned that many problems arise due to a mismatch between individuals and the systems of which they are a part and the role of a social worker is to enhance the fit between the individual and the systems affecting them.
References
Barker, P., 1998. Basic Family Therapy, 4th Edition. Oxford: Oxford University Press.
Beckett, J.A., 1973. General Systems theory, psychiatry and psychotherapy. International Journal of Group Psychotherapy, 23, pp. 292-305.
Benson, M.J; Long, J.K. and Sporakowski, M.J., 1992. Teaching psychopathology and the DSM-III R from a family systems therapy perspective. Family Relations, 41 (2), pp. 135-140.
Bentovim, A. and Bingley Miller, L., 2002. The Assessment of Family Competence, Strengths and Difficulties. London: Pavillion.
Bertalanffy, L. von, 1968. General Systems Theory: Foundations, Development, Application. New York: Braziller.
Bilson, A. and Ross, S., 1999. A history of systems ideas in social work. In, Social Work Management and Practice. London: Jessica Kingsley, 2nd Edition.
Byng-Hall, J., 1988. Scripts and legends in families and family therapy. Family Process, 27, pp. 167-179.
Cecchin, G., 1987. Hypothesizing, circularity and neutrality revisited: an invitation to curiosity. Family Process, 26, pp. 405-413.
Dallos, R. and Draper, R., 2000. An Introduction to Family Therapy. Buckingham: Open University Press.
de Shazer, I., 1982. Patterns of Brief Family Therapy: An Ecosystemic Approach. New York: Guildford Press.
Fleurida, C. et al., 1986. The evolution of circular questions. Journal of Marital and Family Therapy, 12 (2), pp. 112-127.
Goldenberg, I. and Goldenberg, H. , 2004. Family Therapy: An Overview, 6th Edition. London: Brooks/Cole.
Guerin, P.J. and Pendagast, E.G., 1976. Evaluation of family system and genogram. In, P.J. Guerin, ed. Family Therapy. New York: Gardner Press.
James, P. and Murray, R.M., 1991. The genetics of schizophrenia is the genetics of neurodevelopment. British Journal of Psychiatry, 158, pp. 615-623.
Leff, J., 1994. Working with the families of schizophrenic patients. British Journal of Psychiatry, 164 (suppl. 23), pp. 71-76.
O’Brian, C. and Bruggen, P., 1985. Our personal and professional lives: learning positive connotation and circular questioning. Family Prcess, 24, pp. 311-322.
Payne, M., 2002. Systems and Ecological Perspectives. In, Modern Social Work Theory, 3rd Edition. Basingstoke: Palgrave MacMillan.
Penn, P., 1982. Circular questioning. Family Process, 21, pp. 267-280.
Randolph, C., Goldberg, T.E. and Weinberger, D.R., 1993. The neuropsychology of schizophrenia. In, K.M. Heilman and E. Valenstein, eds. Clinical Neuropsychology, 3rd Edition. Oxford: Oxford University Press.
Reder, P., 1983. Disorganised families and the helping professions: “Who’s in charge of what?”. Journal of Family Therapy, 5, pp. 23-36.
Reder, P. and Fredman, G., 1996. The relationship to help: interacting beliefs about the treatment process. Clinical Child Psychology and Psychiatry, 1 (3), pp. 457-467.
Selvini Palazzoli, M.S., Cechin, G., Prata, G. and Boscolo, L., 1980a. Hypothesising-Circularity-Neutrality. Three guidelines for the conductor of the session. Family Process, 19 (1), pp. 3-12.
Selvini Palazzoli, M., Boscolo, L., Cecchin, G. and Prata, G., 1980b. The problem of the referring person. Journal of Marital and Family Therapy, 6, pp. 3-9.
Tomm, K., 1988. Interventive interviewing: part III. Intending to ask lineal, circular, strategic or reflexive questions. Family Process, 27, pp. 1-15.
Reflective Diary Analysis
I applied the theory of psychoanalysis to the practice situation in order to explore underlying issues which had made ME so dependent upon her partner, JM. This appeared appropriate as it would provide an opportunity to gain information about any past experiences which had contributed to her present state, in particular, the nature and origin of her anxieties and fears. Uncovering this information would then inform my practice with ME and JM and provide structure to any intervention.
The overall purpose of psychoanalysis derives from the Freudian assumption that psychopathology develops when people remain unaware of their true motivations and fears and they can be restored to healthy functioning only by becoming conscious of what has been repressed (Bower, 2005). Freud believed that the unconscious conflicts he uncovered – in dreams, in memory lapses, in neurotic symptoms – always referred to certain critical events in the individual’s early life. His observations of his patients led him to conclude that all human beings experience a largely similar sequence of significant emotional events in their early lives and that it is this childhood past that shapes their present (Freud, 1905).
Although Freud cautioned against the use of psychoanalysis in schizophrenia, as he believed that sufferers of schizophrenia had regressed to a state of “primary narcissism”, a phase early in the oral stage before the ego has differentiated from the id (Freud, 1905), more contemporary psychoanalysts have adopted a different approach. Primarily followers of Melanie Klein, they have taken the position that the schizoid position, or splitting between “good” and “bad” objects, was a normal stage of development and that schizophrenia was the late consequence of not negotiating this stage properly (Salzberger-Wittenberg, 1970). Thus, the flow of unconscious material (e.g. delusions, hallucinations and thought disorder) were actively encouraged, explored and participated in.
In ME’s case, a formulation of her presenting issues included the role of specific anxieties and fears. Anxiety has been conceptualised psychodynamically as a state of helplessness and “psychic pain”, which results from the perceived discrepancies between one’s ideal self (or ego ideal) and one’s actual self (Freud, 1926, cited in Brown and Pedder, 1991). These painful discrepancies cannot then be easily assimilated into our conscious view of ourselves and the world because of the anxiety they arouse and the consequence is a “defence mechanism” activated to subdue this psychic pain.
Using open-ended questions with ME, such as “how are you feeling?” and allowing her to respond freely revealed a little of her state of mind, ie. “very low, always tired and very sad”. It was interesting to note ME’s partner, JM’s, explanation of ME’s low mood, “the weather”, a subject he had mentioned at the outset of the encounter. This may indicate an attempt to avoid, or defend against, speaking of difficult issues and furthermore, may represent his own coping strategy. Further questions to elicit ME’s emotional state included “has it made a difference?” (regarding the use of anti-depressants) and “how do you feel about quitting smoking?”
An inherent principle of psychoanalysis is the use of transference and countertransference within any clinical encounter (Casement, 1985; Salzberger-Wittenberg, 1970). Transference is the conveyance of past feelings, conflicts and beliefs into present relationships and situations, spe
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal