Reflection Theories for Nursing Practice
| ✅ Paper Type: Free Essay | ✅ Subject: Nursing |
| ✅ Wordcount: 2377 words | ✅ Published: 23 Sep 2019 |
This essay aims to discuss the principle theories and models of reflection and reflective practice in nursing. The theories of John Dewey and Donald Schön will be deliberated; Dewey regarded reflection as learning by experience through active participation and experimentation, in contrast Schön believed it was both an active and retrospective process. Two models of reflection will also be examined; Graham Gibbs and Christopher Johns. Gibbs (1988) believes there are six stages of reflection, from description of the incident to action plan. John (1995) however has a
five-stage model, each stage has some cue questions that acts as a checklist. Reflection is when you experience a situation, you examine what happened to see if you could have done anything differently or repeat what was successful. Howatson -Jones (2013:6) defines reflection as ‘a way of examining your experience in order to look for the possibility of other explanations and alternative approaches to doing things’. It can also be described as ‘a window through which the practitioner can view and focus self within the context of her own lived experience …’ (Johns, 2010:35). Reflective practice in nursing is looking at the positives and negatives of past decision, learning from this to create a positive outcome in future situations (Japer, 2013).
Theories of reflection can be described as different questions which helps to clarify your knowledge. Models of reflective practice are questions that allows peoples experience to be evaluated by applying previous knowledge to your work. It can be argued that, the history of reflection in Nursing is not a recent phenomenon One of the first reflective theorists is an American psychologist Dewey (1938). He believed much of our learning is derived from our experiences and experimenting with ideas. Dewey (1938, cited in Rolfe, Jasper and Freshwater 2011:34) ‘we learn by doing and realising what came of what we did’. Dewey’s created the model of reflective learning, this consists of three stages. First, we experience the situation, secondly, we observe and reflect on it, thus we gain a better understanding of the event. Thirdly, the deep comprehension turns into knowledge. (see figure 1) Dewey defined reflection as (1933:9 cited in Bulman and Schutz 2013:2) ‘Active, persistent and careful consideration of any beliefs or supposed form of knowledge…’ He viewed reflection as a scientific process of thinking for a purpose, it requires focus on knowledge adjusting and experimenting with idea accordingly (Bulman and Schutz 2013:2).
Schön (1988) is another influential figure, in the history of reflection. His work was developed from Dewey’s idea, from this he created a two-stage theory: reflection- in- action and reflection- on -action. Reflection-in-action means thinking about the action whist performing the task or procedure and actively amending one’s action accordingly. Schön emphasises that thinking on your feet, was key to producing the expert practitioner. Schön (1983:163, cited in Johns 2017:7) ‘he shapes it and makes himself part of it’. Reflection-on- action is concerned with examining the experience in greater detail after it has happened, finding alternative ways to do something to achieve the best possible outcome (Jasper, 2013). A criticism of this model is that it is very vague, it does not offer any checklist questions to guide reflection. It relies on the individuals interpretation only, it can be argued that it is difficult to measure the effectiveness.
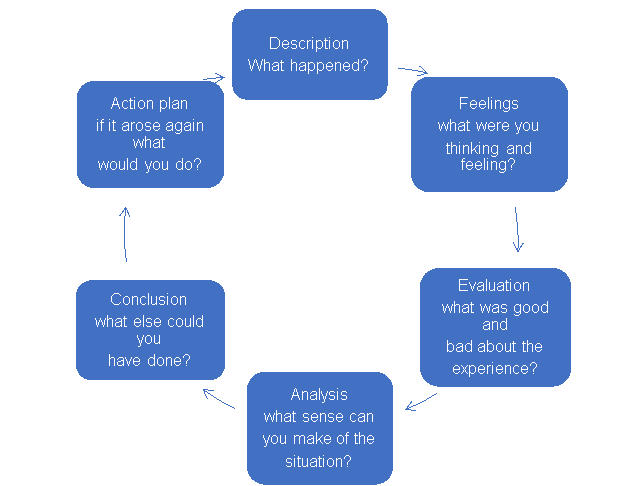
This section will compare 2 models of reflective practice in greater depth. Gibbs (1988) six stage Reflective cycle, is based on Dewey’s (1938) model. The first stage is the experience, this is where you recall the critical incident and analyse your reaction of the event. The second stage deals with the feeling, you discuss your emotions, in terms of what you were thinking and how you felt at the time. Next you analyse, by exploring what went well and what did not go as planned. Then you discover areas of improvement in your Skills, which the enables further learning. This leads on to the conclusion phase where you make a judgement with the information you have gathered on this exercise. These could be both success or failure from this, you develop an action plan, which is the last phase in this model. (see figure 2). Gibbs believes that feelings and emotions significantly influence actions, therefore understanding self is key to reflective practice. The key strength of this model is that it is clear, concise and straight forward to use. It is suitable for both the novice and the experienced professional. One criticism of this model is that there are some nuances, between the evaluation and analysis steps. This is exemplified in the question, what was good or bad and what else can you make of this experience. This is essentially asking the same question, in different ways which could lead to confusion.
Johns developed Model of Structured reflection (MSR, 1995) based on Barbara Carper’s (1978) fundamental patterns of knowing. Which contained 4 phases: empiric (measurable actions), personal(self-awareness), ethical (moral knowledge) and aesthetics (whole picture). Johns MSR has five phases, with some cue questions together with the influence grid to enable greater analysis of each phase (see figure 3&4). He has since revised the MSR (2010 and 2015) in each occasion adding more clarity to the steps. The first phase is the preparatory, which he refers to as ‘bring the mind home’ this basically mean focus on the significant experience. Secondly, the focus then leads on to the descriptive phase, where you describe the experience and what issues were significant. Thirdly, the reflective phase asks you to consider the internal feeling and external influencing factor of the decisions, this considers your own and other people’s feelings. This is primarily trying to ascertain if your actions were influenced by others and if you acted differently because of this. The fourth phase is the anticipatory, which ask you to speculate how you would have changed the situation, if there was any constraint stopping you and how this might have affected the outcome. It also prompts you to evaluate the incidence retrospectively, the fifth phase is the insight, which concerned with what knowledge has been achieved as a result. Johns believes when reflecting on our performances, it is necessary to consider internal and external influencing factors (Jasper, 2013). And without this individual cannot transition to reflective practice. The strengths of this model are that the questions are very specific, this is exemplified in the question what you were trying to achieve, this can assist your reflection. Another positive is that it has been modified severally, which show the model is truly reflective. The main weakness with this model is that there too many questions to consider in each stage, this might lead to confusion, especially for the newly qualified practitioner, who might not have enough insight into own knowledge in order to analyse it extensively. The influence grid might also be distracting from real thoughts, therefore influencing your answers.
There are several similarities between Gibbs and Johns reflective models, the first is the learning outcome of the experience which is the analysis, the second point is what you will approach differently next time, known as the action plan. There are some important differences between Gibbs and Johns models. Johns MSR uses cue questions and an influence grid to prompt the Practitioner to include, external factors such as other people’s feelings, which might have influenced their decisions. Gibbs model in contrast uses an individualised approach, the focus is on the practitioner’s thoughts only, it is not concerned about other people’s influences. Another difference is that Gibbs ask you to evaluate your approach to work, however Johns is only concerned with what you have learnt from the experience or will change in future.
Reflective models can be applied in practice by utilising the strategies to support some of the key challenges facing nurses. For example, the rise in physical assault on nurses from service users. A recent report on (BBC, 2017) violence in the work place, identified that there were nearly 200 attacks on health care workers daily in England. Gibbs model can be used in this scenario, the professional will be able to spot the triggers in advance. He would communicate effectively with the patient to de-escalate and resolve the issues. Another problem in nursing is drug errors, a study by Westbrook et al (2010, cited in Nursing standard, 2018 vol33:59) identified that 25% of all medicines administration by nurses had one clinical error. The Nursing and Midwifery council (2007) nine rights of medicine Administration, together with Schön’s reflection -in -action- theory could be applied to this scenario (Schön, 1983, cited in Martin 2013) by having an action plan and clear strategies. The professional would actively double check the medication and any errors would be identified, rectified before administering to patient. NMC (2018), states that all nurses, must uphold professional standards know as ‘The code’: prioritise people, practise effectively, preserve safety, promote professionalism and trust. Johns MSR model (2015) can be utilised here to identify gaps in knowledge, generate an action plan to address these issues. Reflective practice thus supports key principle of the National Health Service (NHS 2012), code of conduct known as the 6C’s: care, compassion, competence communication, courage and commitment.
Having emphasised the relationship between reflective theories and models been an essential tool to establish reflective practice. I am now going to reflect in this section on a critical incidence, applying the Gibbs model. I was waiting patiently in an open-air carpark queue. I had been waiting for just over twenty minutes, when I reached the front of the queue. I was feeling quite pleased that at last the wait would be over as I saw a shopper leaving a parking space. suddenly a car about few spaces behind the queue reversed, drove through a no entry route and manoeuvred into the space. I was feeling angry, shocked and annoyed that this woman can just jump the queue. I went over and told her calmly, that there was a queue system and that the space was mine. She pretended she could not understand what I was saying at first, then she claimed to have been approached by the previous driver to park there and did not see the queue. She refused to move, parked up and paid for her ticket. The negative part of this incidence was that I had to wait an additional ten minutes to find a space, another negative was that I kept seeing her round every shop I went into that afternoon. This ruined my shopping experience, because for majority of the time I felt uncomfortable even though I had been in the right. I had to accept that I could not change other people’s behaviour, I could only change mine. I can conclude from this experience that it was pointless trying to explain the situation as it did not achieve my main goal. My action plan would be, to avoid confrontation in the future but instead wait for another parking space or find another carpark.
This essay has examined the reflective theories of Dewey and Schon and the models of Gibbs and Johns. When comparing the theories and models it became obvious that each situation might determine the choice of reflection. For example, Schön’s theory might be suitable for the experienced nurse whilst Dewey’s could be appropriate for the novice. Johns model might be best for deeper analysis on the other hand Gibbs favours a straightforward approach. It remains clear that theories and models are useful, in the transition to professional behaviour in nursing practice. By identifying strengths and weakness and creating an action plan it can enable personal growth and competence in skills. It can Improve patient safety by preventing errors, promote person centred care, as self-awareness is a key element of reflection. Reflective practice also supports the 6C’s (NHS, 2012) and (NMC 2018) ‘the code’. It can be applied in different situation however it is relevant to remember to use them wisely and apply common sense. John (2017:36) reminds us that ‘models are not a prescription for reflection’.
References
- BBC (2017) NHS Health check ‘most staff have been attacked; doctor says’ available at https://www.bbc.co.uk/news/health-38917156 accessed 19 December 2018.
- Bulman, C .and Schutz, S. (2013) Reflective Practice in Nursing edn:2 Oxford: Willey-Blackwell.
- Howatson-Jones, L. (2013) Reflective practice in Nursing edn:2 London: Learning Matters.
- Jasper, M. (2013) Beginning reflectively practitioner edn:2 Andover: Cengage learning.
- Johns, C. (2010) Guided reflection edn:2 Chichester: Wiley-Blackwell.
- Johns, C. (2017) Becoming a reflective practitioner edn:5 Chichester: Wiley-Blackwell.
- Johns, C. (2017) MSR fig3, influence grid fig.4, p.37-38. Becoming a reflective practitioner edn:5 Chichester: Wiley-Blackwell.
- Martin, P. (2018) Coping and thriving in nursing London: Sage publication.
- National Health Service (2012) ‘The 6C’s’ available at www.england.nhs.uk/leadingchange/6cs.
- Nursing and Midwifery Council (2007) Standards for Medicine Management: London. Available at https://www.nmc.org.uk/standards-for-medicine-management Accessed 24 December 2018.
- Nursing and Midwifery Council (2018) ‘The code’: professional standards of practice and behaviour for nurses, midwives and nursing associates: London available at https: www.nmc.org.uk/standards/ code. Accessed 24 December 2018.
- Nursing standards Understanding the Human and System Factors involved in Medication errors vol (33) pp.59-61 September 2018.
- Rolfe, G. Jasper. Freshwater, D. (2011) Critical reflection in practice edn:2 Basingstoke: Palgrave Macmillan.
- Rolfe, G. Jasper. Freshwater, D. (2011) ‘Dewey’s model of reflective learning’ (1938) Critical reflection in practice edn:2 p.34 Basingstoke: Palgrave Macmillan.
- Rolfe, G. Jasper. Freshwater, D. (2011) ‘Gibbs reflective framework’ (1988) Critical reflection in practice edn:2 p.35 Basingstoke: Palgrave Macmillan.
- Siviter, B. (2013) The student nurse handbookedn:3 London: Elsevier.
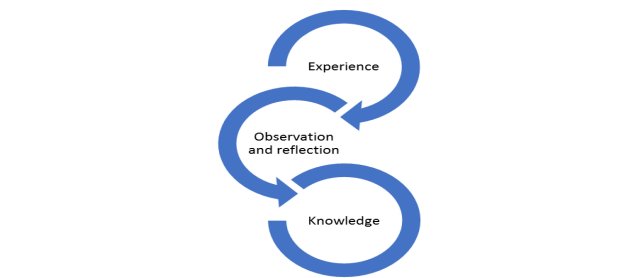
Sourcefig.1: Rolfe, Jasper& Freshwater. 2011:33
Appendices
Figure 1: Dewey’s model of reflective learning (1938)
Source: fig.2 Rolfe, Jasper & Freshwater 2011:34
Figure 3: Johns model for structured reflection (MSR) edition 17th.
Figure 2: Gibbs reflective framework
Reflective cue
Appendix 3 The
Source: Johns, 2017
Bring the mind home
Write a description of an experience
What in particular seems significant to pay attention to?
Why did I respond as I did?
Was I effective in terms of consequences for others and myself?
What factors influenced my response (see figure 4)
Given the situation again, what are my options for responding more effectively?
What are the potential consequences of responding differently?
How do those influencing factors need to shift so I can respond differently?
What tentative insight do I draw?
How does extant theory/ idea inform and deepen my insights?
How does exploring with guides and peers challenge my insight?
How do I feel now about the situation?
Source fig. 3: Johns 2017:37
Source Johns 2017:37
Appendices
Figure 4: Johns Influence Grid
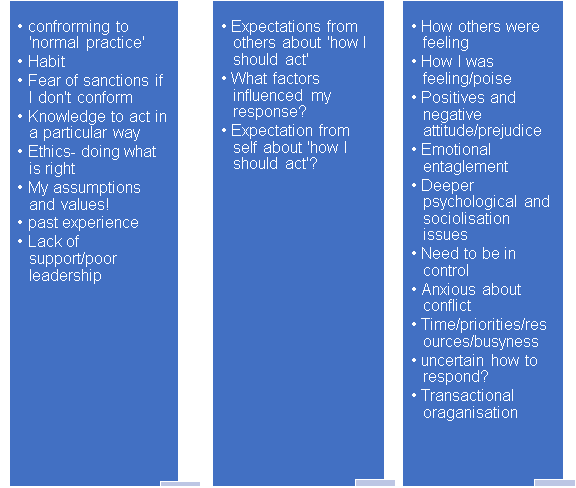
Source Fig.4: Johns 2017:38
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal