A practical guide to health promotion assignments
Info: 4789 words (19 pages) Study Guides
Published: 17 Mar 2026
Still struggling with your health promotion assignment? We can help! Our team is qualified and ready to assist with your writing projects. Check out the nursing assignment help page for more info.
Health promotion assignments in nursing require students to design effective patient education materials or community health programmes. These tasks assess understanding of public health principles, health promotion strategies, and behaviour change theories.
The nurse’s role as a health promoter is emphasised by professional standards. The Nursing and Midwifery Council (NMC) Code instructs nurses to “pay special attention to promoting wellbeing [and] preventing ill health” across all life stages (NMC 2018). In practice, this means every interaction is an opportunity to educate patients and communities about healthier choices.
Health promotion is defined by the World Health Organization (WHO) as “the process of enabling people to increase control over, and to improve, their health” (WHO 1986). This broad definition underlines that effective health promotion goes beyond treating illness. It empowers individuals and communities to manage their health, addresses social determinants of health, and involves multi-level interventions.
In an assignment, you must demonstrate a clear grasp of these concepts and apply them to a realistic scenario, such as reducing smoking among teenagers, in a structured, evidence-based way. This guide outlines how to approach such assignments, including planning a health promotion programme, integrating behaviour change theory, and developing patient education materials, all in the context of UK nursing practice.
Understanding health promotion and public health context
Why the public health context matters
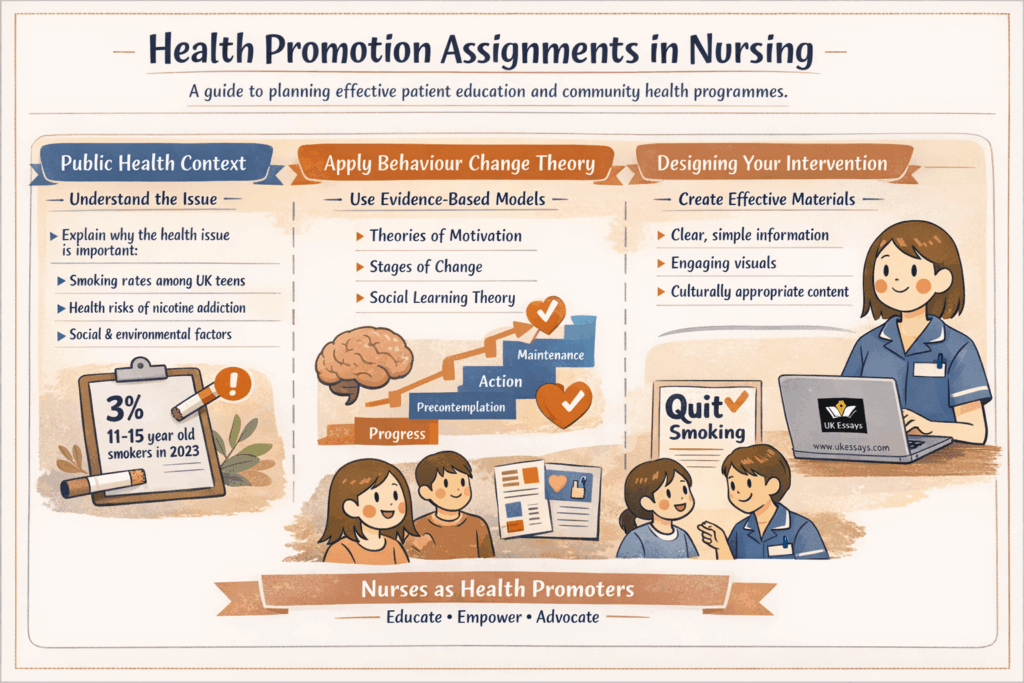
Before planning the intervention, ensure you explain the public health context of the issue. Health promotion is fundamentally about improving population health and reducing health inequalities. It is rooted in public health principles such as prevention, equity, and community engagement.
For example, an assignment on teenage smoking cessation should explain why adolescent smoking is a public health concern. Early nicotine addiction leads to long-term health risks, and smoking prevalence in UK teenagers, though relatively low, still means thousands of young people are affected. Citing current data can strengthen your case. For instance, around 3% of 11–15-year-olds in England were current smokers in 2023 (NHS Digital 2024).
Such statistics illustrate the scope of the problem and justify the need for intervention. You should also consider wider determinants. Factors such as peer pressure, family environment, socio-economic status, and education level all influence the health behaviour in question.
A high-quality assignment will show awareness that effective health promotion must address not only individual behaviour but also these broader influences on health.
Policy and professional context
It is also useful to refer to national health strategies or guidelines that frame the issue. UK health policy documents, such as tobacco control plans or youth health strategies, often set targets and recommend approaches. Mentioning these shows the assessor that you understand the issue in context.
For example, you could note that the assignment’s aims align with Public Health England’s “All Our Health” framework on smoking prevention, which encourages evidence-based interventions in schools and communities. By situating your programme within such frameworks, you demonstrate a public health perspective and awareness of current best practice.
Remember that health promotion in nursing is not an optional extra. It is a core responsibility. Nurses are expected to advocate for healthy lifestyles, educate patients, and collaborate in public health efforts (NMC 2018). Your assignment should therefore reflect the nurse’s proactive role in improving health and preventing illness at both individual and community levels.
Approaches and strategies for health promotion
Overview of the main approaches
When designing a health promotion intervention, it is important to outline the approach or approaches you will use. Health promotion literature describes several classic approaches, each with distinct aims and methods (Phillips 2019).
Medical or preventive approach
The medical or preventive approach focuses on disease prevention through medical interventions such as immunisations, screenings, and early detection. In a smoking cessation context, this might involve offering nicotine replacement therapy or screening for smoking-related illness.
However, this approach alone is often top-down. It may also overlook psychosocial factors that shape behaviour.
Behaviour change approach
The behaviour change approach encourages individuals to adopt healthier habits through persuasion and education. For example, a behavioural approach to teenage smoking might use campaigns to persuade young people not to start smoking, or to quit if they have already started.
The aim is to change personal habits. This might be done by highlighting immediate drawbacks of smoking, such as reduced sports performance or financial cost, to motivate change.
Educational approach
The educational approach provides information and develops understanding so people can make informed decisions about their health. It is about empowering through knowledge without coercion.
In your programme, an educational session might teach teenagers about the effects of tobacco, the benefits of quitting, and ways to resist peer pressure. The tone should be enabling rather than dictating, and the content should be age-appropriate and engaging.
Empowerment approach
The empowerment approach enables people or communities to take greater control over their health by building skills, confidence, and social support. It is often client-centred and participatory.
For a youth smoking initiative, this could involve peer-led support groups or training youth ambassadors as anti-smoking champions. The aim is to boost self-efficacy and give the target group ownership of the intervention. For example, teenagers could be involved in co-creating campaign messages that resonate with their peers.
Social change approach
The social change or societal approach advocates for environmental and policy changes that make healthy choices easier. Even in a student assignment, you should still consider the environment or local policy context.
For instance, you might propose working with schools to enforce no-smoking policies on campus or calling for tighter restrictions on youth access to vaping products. This approach addresses the wider context rather than the individual alone (Phillips 2019).
Combining approaches
In practice, effective health promotion programmes often combine approaches. Your assignment might mainly describe an educational programme, but still include elements of empowerment and social change.
For example, a community-based teen smoking reduction programme might include informative school workshops, a peer mentoring scheme, and collaboration with local authorities to create smoke-free zones around youth centres. Make it clear which strategies you are using and why. This shows critical thinking and gives your intervention a clear rationale.
You might write: “In addition to delivering educational sessions to raise awareness about smoking harms, the programme will train volunteer teenage ‘health champions’ to provide peer support, an empowerment strategy chosen to leverage peer influence in a positive way (Phillips 2019).” Linking each strategy to theory and evidence will strengthen your assignment.
Planning a health promotion programme step-by-step (H2)
Aims and objectives
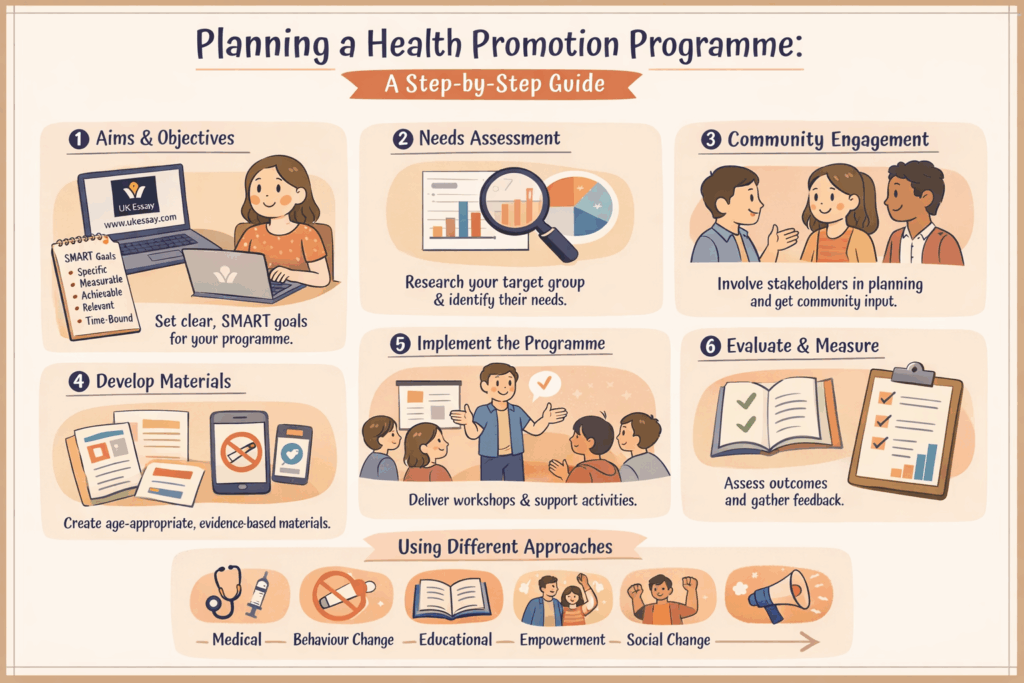
A logical, structured plan is the backbone of your assignment. Start by clearly defining the aims and objectives of your health promotion initiative. The overall aim is the broad goal, such as reducing the prevalence of cigarette smoking among teenagers in a given community.
Objectives should be SMART: specific, measurable, achievable, relevant, and time-bound. For example, an objective could be “to decrease the percentage of 15-year-old pupils at Greenwood School who smoke regularly from 5% to 2% within one year.” Well-crafted objectives provide focus and allow outcomes to be evaluated.
They also show your marker that you understand how to measure success in health terms, whether through changes in knowledge, attitudes, or behaviour.
Needs assessment
Next, conduct a needs assessment, at least hypothetically within the assignment’s scope. This means using data and evidence to justify your approach. Describe the target population and explain why they need this intervention.
This could include epidemiological data, but also evidence from literature about risk factors or barriers. For instance, you might note that most smokers start in adolescence, and that peer influence and tobacco advertising on social media are contributing factors.
If available, include local data or realistic scenario-based insights. You might refer to a school health survey showing that 30% of students had tried vaping. Even if you create a scenario, it should still be grounded in evidence. A good needs assessment may also consider existing resources or services, such as local stop-smoking support for young people, and identify any gap your programme could fill.
Preparation and community engagement
Once the background is established, outline the intervention activities in a logical sequence. Begin with preparation and community engagement. Explain how you will involve stakeholders in the planning process.
In a teen smoking programme, these stakeholders might include schools, parents, youth workers, public health teams, and the teenagers themselves. You could propose initial meetings or focus groups to gather input and ensure the programme is culturally and socially appropriate.
Engaging the target audience in planning, perhaps through a youth advisory panel, can improve both relevance and uptake.
Development of materials and messages
If you are creating educational content such as leaflets, presentations, or social media posts, describe this process clearly. State that materials will be evidence-based, age-appropriate, and attractive to the target audience.
You could also mention using clear language and visuals, and pre-testing the materials with a small group of teenagers for feedback. This demonstrates a methodical and user-centred approach to intervention design.
Implementation of the intervention
Then explain what will happen, where, and when. For example, you might write: “Starting in September, weekly interactive workshops will be delivered in the community youth centre and at local secondary schools over a 3-month period.”
Describe each component clearly. This may include educational sessions on the short-term and long-term effects of smoking, practical skills training such as role-play to resist cigarette offers, and support mechanisms such as a confidential text helpline or drop-in clinic with the school nurse.
Keep the description concise, but detailed enough to show that you have considered practicalities. Mention who will deliver each part and what resources are needed. For example, school nurses and trained peer educators might co-facilitate sessions. You might also need venues, printed materials, or small incentives such as healthy snacks or recognition awards.
Collaboration and partnerships
Highlight any collaboration with existing services or professionals. For example, you might work with local stop-smoking services, perhaps asking a cessation counsellor to run selected sessions or provide quitting aids for those ready to stop.
You could also align with a national campaign, such as NHS Smokefree resources, where appropriate. This shows the programme is not working in isolation. It draws on existing expertise and public health infrastructure.
Evaluation plan
An assignment should always explain how you will evaluate success. Consider both process evaluation and outcome evaluation. Process evaluation asks whether the activities were delivered as planned, how many people attended, and how engaged they were. Outcome evaluation asks whether the programme met its objectives.
For a teen smoking example, outcomes could be measured through follow-up surveys on smoking rates or intentions after the programme. You could also measure changes in knowledge through pre- and post-session quizzes, or changes in attitudes through questionnaire responses.
It is useful to include at least one quantitative measure, such as a percentage change in smoking or an increase in knowledge scores, and possibly some qualitative feedback from focus groups. Mentioning a longer-term follow-up, perhaps six months later, is also good practice.
Throughout this section, use active voice and clear language. A well-structured plan shows that you can translate theory into practical action in a systematic way.
Integrating behaviour change theories
Why theory matters
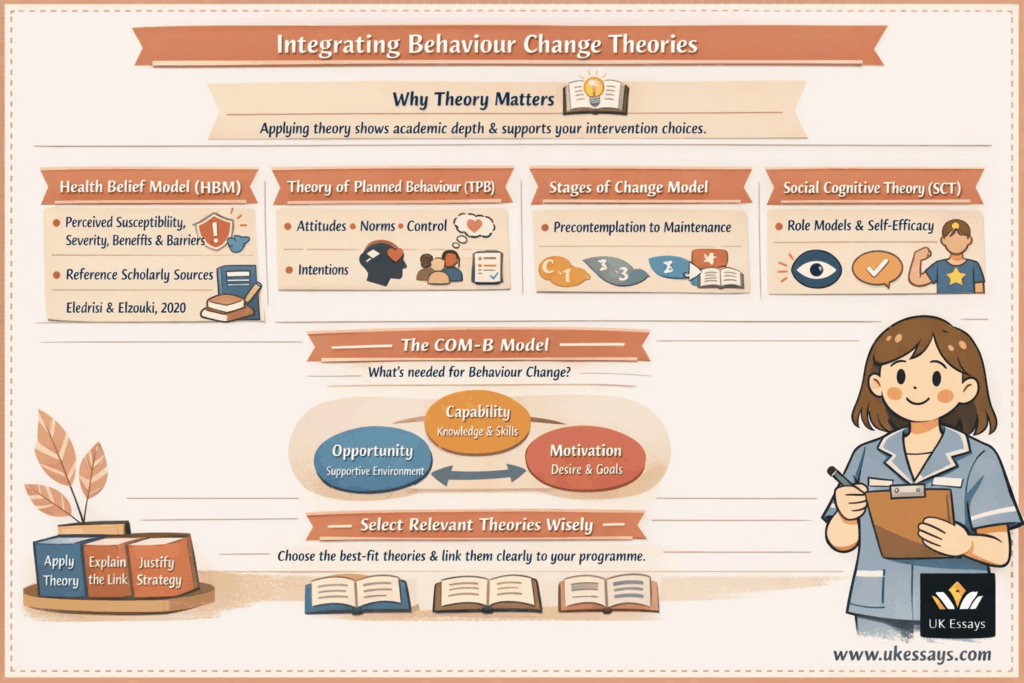
A strong health promotion assignment will explicitly connect the programme design to behaviour change theory. Theories help explain why people engage in unhealthy behaviours and how they change them. Demonstrating theoretical underpinning shows academic depth and helps justify your intervention choices.
Health Belief Model (HBM)
The Health Belief Model suggests that people are more likely to take health action if they feel susceptible to a problem, believe it could have serious consequences, see benefits in action, perceive fewer barriers, and receive cues to act (Rosenstock 1974).
In your programme, you might apply HBM by showing teenagers their susceptibility to addiction and the immediate effects of smoking on fitness, appearance, and lung health. You would also make the benefits of not smoking clear, such as saving money or improving sports performance, while addressing barriers like fear of social exclusion.
A cue to action could be a pledge or a school-wide no-smoking challenge. You might write: “The educational materials will emphasise the serious health risks of smoking, raise awareness of addiction, and highlight the benefits of quitting while offering solutions to common barriers such as nicotine cravings, an approach informed by the Health Belief Model (Rosenstock 1974).”
Theory of Planned Behavior (TPB)
The Theory of Planned Behavior argues that behaviour is driven by intention. Intention is shaped by attitudes, subjective norms, and perceived behavioural control (Ajzen 1991).
In practice, your programme might challenge misconceptions by showing that most teenagers do not smoke. It could also use relatable role models to promote positive attitudes towards a smoke-free lifestyle. To improve perceived behavioural control, you might teach refusal skills and show students how to access support.
For example, you could write: “The programme will apply the Theory of Planned Behavior by targeting attitudes through peer-led discussion, subjective norms through positive messaging about non-smoking, and perceived behavioural control through role-play and problem-solving exercises” (Ajzen 1991).
Transtheoretical Model (Stages of Change)
The Transtheoretical Model identifies stages in behaviour change, including precontemplation, contemplation, preparation, action, and maintenance (Prochaska and DiClemente 1983). This is useful because not all participants will be equally ready to change.
Some teenagers may not have thought about quitting at all, while others may already be trying. You can therefore tailor the intervention to different stages. General awareness campaigns may suit those in precontemplation, while one-to-one advice or quit plans may better support those preparing to stop.
A strong assignment might note that posters and assemblies target those not yet considering change, while small-group workshops and follow-up support help those in the action or maintenance stages.
Social Cognitive Theory (SCT)
Social Cognitive Theory highlights the role of observational learning, imitation, and self-efficacy. People are more likely to adopt behaviours they see modelled by people they admire.
In a teen smoking programme, this supports the use of peer role models, youth ambassadors, or local sports figures who model a healthy, smoke-free lifestyle. It also supports activities that build confidence, such as practising how to say no in realistic situations.
Even if you do not explore SCT in detail, referring to the importance of self-efficacy and role modelling will still show theoretical understanding.
COM-B model and Behaviour Change Wheel
The COM-B model proposes that behaviour is shaped by Capability, Opportunity, and Motivation (Michie et al. 2011). To change behaviour, an intervention should strengthen all three.
In this example, capability would involve knowledge about smoking harms and practical refusal skills. Opportunity would include supportive school environments, smoke-free spaces, and access to help. Motivation would be shaped through peer encouragement, positive messaging, and personal goal-setting.
You might write: “The intervention was designed using the COM-B framework, ensuring participants develop capability, have greater opportunity, and build motivation to remain tobacco-free” (Michie et al. 2011).
Using theory selectively
Linking to one or two theories is usually enough. The aim is not to mention every theory, but to show that you can apply the most relevant ones well.
Choose the models that best fit your programme and explain clearly how they influenced your design. This shows that you are not proposing random activities. You are selecting strategies because theory and evidence suggest they are likely to be effective.
Designing effective patient education materials
Clarity and simplicity
If your assignment involves creating patient education materials, such as a leaflet, poster, or digital infographic, you should give careful attention to health communication principles. Well-designed materials can strengthen your programme by informing and motivating your audience.
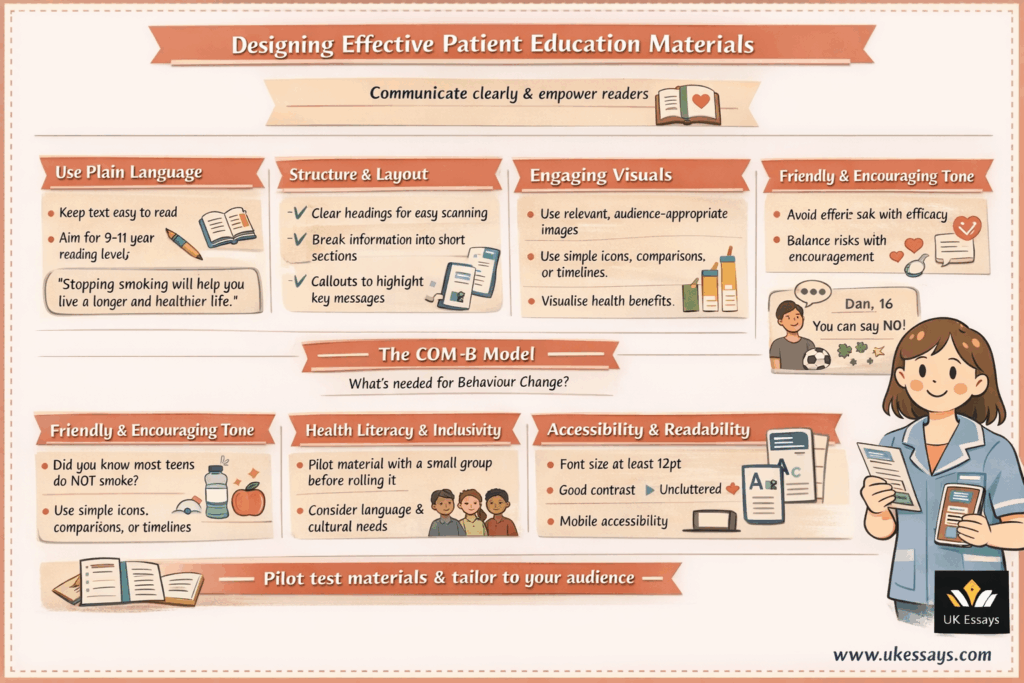
Use plain language and avoid jargon. Health literacy levels vary widely, and many adults in the UK struggle with standard health information (Patient Information Forum 2022). Aim for a reading age of roughly 9–11 years. This means short sentences, familiar words, and simple explanations of any essential medical terms.
For example, instead of saying “Smoking cessation reduces morbidity and mortality,” you could say “Stopping smoking will help you live a longer and healthier life.” The tone should be respectful, clear, and empowering.
Structure and layout
Organise content with clear headings and easy-to-follow sections so information can be scanned quickly. Use sentence case for headings, and make the most important messages stand out through restrained bolding or a simple call-out area.
Paragraphs in a leaflet should be short. Avoid dense blocks of text. Each section can focus on a common question or theme, such as why smoking is harmful, the benefits of quitting, how to get help, or how to deal with cravings. A clear structure helps guide the reader from awareness to action.
Engaging visuals
Relevant images or graphics can increase engagement and understanding. For a teenage audience, visuals might include healthy activities, simple comparisons, or a basic infographic showing how quickly health improves after quitting.
Images should support the text and suit the audience. Avoid imagery that is so frightening or stigmatising that it becomes counterproductive. Visuals should inform, not overwhelm.
Tone and empowerment
The material should feel encouraging and relatable. For teenagers, a more conversational tone may work well. For example: “You might think everyone your age has tried smoking, but most young people do not smoke. You are not odd for saying no.”
Include positive messages about the reader’s ability to change. Avoid relying only on guilt or fear. Instead, balance risk information with clear encouragement and realistic benefits. Where appropriate, short peer testimonials can make the material feel more relevant.
Health literacy and inclusivity
A good assignment will show awareness of health literacy and inclusivity. You can state that you would pilot the material with a small focus group from the target audience to check whether it is clear, appealing, and easy to understand.
You should also consider language barriers, literacy difficulties, and cultural relevance. If the target community is diverse, you might mention translations or greater use of visual communication. Everyday examples are usually more effective than technical wording (Patient Information Forum 2022).
Design details and accessibility
Use a readable font such as Arial or Calibri in a suitable size. Ensure good contrast between text and background. Do not overcrowd the page. White space helps make information feel manageable and easier to read.
If the material is digital, mention accessibility on mobile devices and any useful interactive elements, such as a short quiz. If it is printed, explain how the layout avoids becoming text-heavy.
Credibility and support
Educational materials should also feel credible. Briefly indicating trusted support sources, such as NHS services, can build trust. It is also important to show where the reader can get more help.
This might include a helpline, an app, or contact details for a school nurse or youth clinic. For teenagers, it can also help to mention whether support is confidential. That reassurance may increase the chance that someone seeks help.
By discussing how you would create and use patient education materials, you demonstrate practical health promotion skills. You also show that communication is part of the intervention itself, not just an afterthought.
Example application: reducing smoking among teenagers
Scenario context
To show how these ideas fit together, consider the example: “Develop a community-based education programme aimed at reducing smoking among teenagers.”
You are a public health nursing student working in a small town in England. Local data suggests that although adult smoking rates have fallen, a concerning number of younger teenagers are experimenting with cigarettes and e-cigarettes. The community has two secondary schools and several youth clubs, but no dedicated anti-smoking initiative for young people.
Aims and objectives
The aim of the programme is to prevent smoking uptake and support current young smokers to quit, thereby reducing tobacco use among local teenagers.
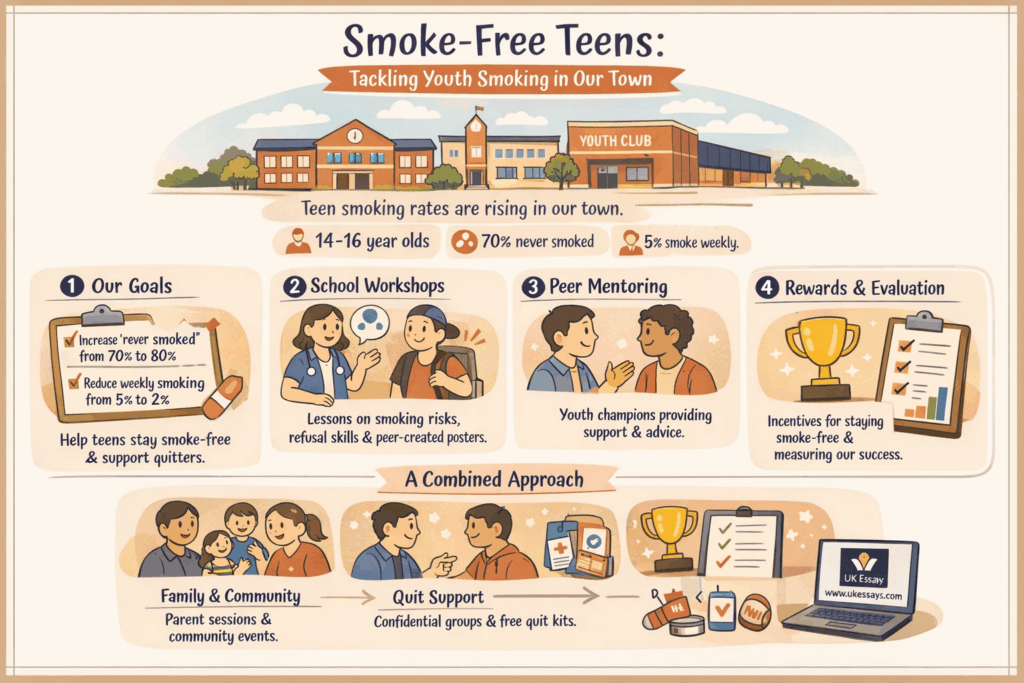
One SMART objective could be: “By the end of the 6-month programme, increase the percentage of 14–16-year-olds in the community who report ‘never smoking even a puff’ from 70% to 80%, and reduce the number who smoke weekly from 5% to 2%, as measured by an anonymous survey.” A second objective might focus on knowledge, such as increasing the proportion of participants who can identify key harms of smoking and benefits of quitting.
Programme design
Named “Smoke-Free Teens”, the programme would run in collaboration with local schools, the youth centre, and the council’s public health team. It would combine educational, behavioural, and empowerment approaches.
This combination is useful because it allows the programme to inform, motivate, and support teenagers rather than relying on one method alone.
Stakeholder engagement
The first stage would involve meetings with school leaders, teachers responsible for PSHE, parent representatives, and youth workers. Their support would help with scheduling, community access, and communication.
Input should also be gathered from students. This could be done through a short anonymous survey or student council discussion about attitudes to smoking and the influences behind it. This step also acts as a needs assessment. The local Stop Smoking Service could be approached for expertise and practical resources.
Educational sessions in schools
Over one school term, workshops could be delivered to Year 9 and Year 10 pupils. A public health nurse and a trained young volunteer might co-facilitate these sessions to keep the tone more peer-friendly.
One workshop could focus on understanding smoking risks through quizzes and myth-busting. Another could build refusal skills through role-play and discussion. A third session might explore healthier ways to cope with stress and social pressure. A final session could ask students to create anti-smoking posters or social media messages, reinforcing learning while also spreading peer-led content.
Peer mentoring and support
The programme could recruit volunteer Youth Health Champions from older students. They would receive training in smoking knowledge, confidentiality, listening skills, and when to refer concerns to adults.
These champions could then support younger students informally, help at school health events, and take part in awareness campaigns. This peer-led element reflects empowerment principles and the idea that adolescents may respond more positively to near-peers than authority figures.
Family and community component
Because families and communities influence teenage behaviour, the programme should not focus only on schools. An evening session for parents could explain how to discuss smoking at home, spot signs of vaping or smoking, and find support
The youth centre could also be involved. For example, it might host a mural project, poster competition, or public event themed around healthy lungs and smoke-free living. This helps build wider community visibility and supports a norm that smoking is not valued.
Use of educational materials
Throughout the programme, tailored materials would reinforce key messages. A colourful leaflet, designed with student input, could summarise smoking harms, benefits of quitting, available support, and the fact that most young people do not smoke.
The leaflet could also include short local testimonials and simple statistics. For example: “In England, only 3% of 11–15-year-olds smoke regularly, so if you do not smoke, you are absolutely normal” (NHS Digital 2024). Posters created by students could be displayed in schools and community settings, while a simple social media campaign could extend the message online.
Behavioural supports
For teenagers who already smoke and want to quit, the programme could offer a weekly confidential support group. This might be led by the school nurse or youth worker and use motivational interviewing techniques.
Free quit kits could also be offered through the local Stop Smoking Service. These might include practical tip cards, stress-relief items, and, where appropriate, access to nicotine replacement therapy with proper safeguards. This shows the programme supports both prevention and cessation.
Incentives and reinforcement
Teenage programmes often benefit from visible reinforcement. A “Stay smoke-free for 30 days” pledge could be used to build momentum. Participants who remain smoke-free could be entered into a prize draw for something meaningful, such as sports equipment or a gym pass.
These incentives should remain secondary to the health message. They can help start engagement, but the programme should still focus on long-term motivation and behaviour change.
Theory in action
Throughout this design, theory shapes practice. The programme uses HBM by highlighting risk and benefits, addressing barriers, and creating cues to action. It uses TPB by influencing attitudes, social norms, and perceived control.
It also reflects stages of change by offering different forms of support for people at different levels of readiness. COM-B is evident too. The programme builds capability through education and skills, improves opportunity through support and smoke-free environments, and strengthens motivation through peer influence, goal-setting, and encouragement.
Evaluation
The programme should end with a clear evaluation plan. A baseline survey in both schools could measure smoking and vaping behaviour, attitudes, and knowledge before the intervention begins. The same survey could then be repeated at the end of the school year.
Participation should also be tracked, including workshop attendance and engagement with quit support. Qualitative feedback from student focus groups could help explain what worked well and what did not. If smoking rates fall and student responses are positive, the intervention could be considered effective. If results are limited, the assignment should reflect on why and suggest changes for future improvement.
This example shows how theory, planning, communication, and evaluation can be integrated into one coherent health promotion assignment.
Conclusion
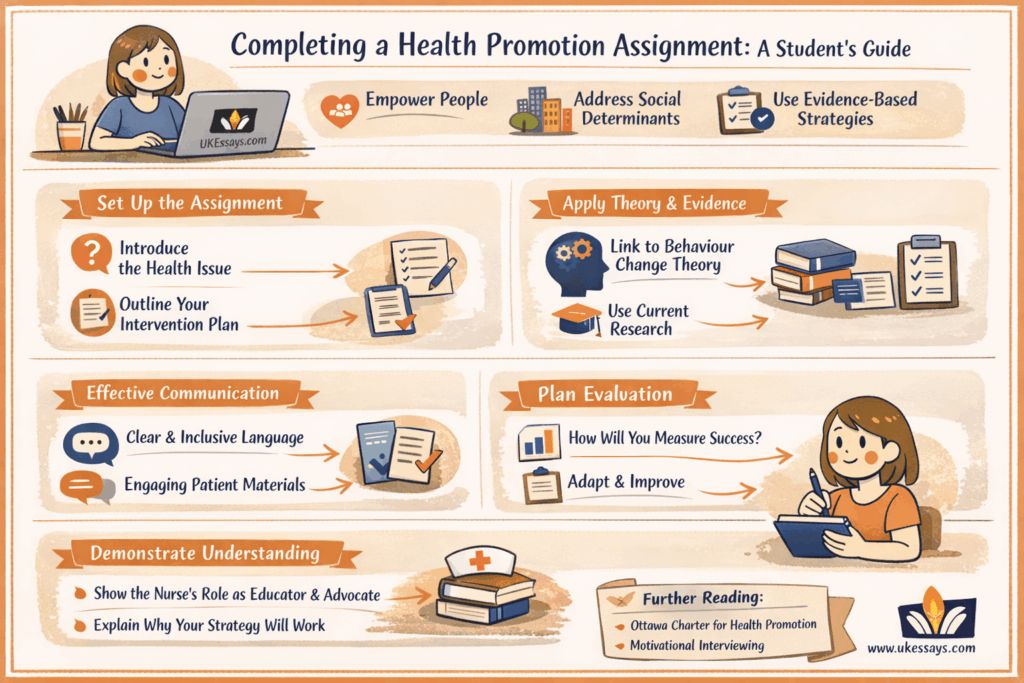
In summary, completing a health promotion assignment involves blending academic understanding with practical planning. Start with the core principles: empower people, address the wider determinants of health, and use evidence-based strategies to encourage healthier behaviour. Make sure you also highlight the nurse’s role as a health educator and advocate. In the UK, this is not just good practice. It is a professional duty (NMC 2018).
Structure the assignment clearly. Introduce the health issue and explain why it matters. Then describe your planned intervention step by step. Use headings and logical flow to guide the reader.
Always underpin your plan with behaviour change theory and current evidence. This turns a simple proposal into a stronger academic piece. For example, do not just state that you will educate teenagers about smoking. Explain how this is expected to influence beliefs, intentions, and behaviour in line with theory.
Pay attention to communication techniques, especially when designing patient materials. The success of any health message depends partly on how clearly and sensitively it is delivered. Mention the need for accessible language, appropriate tone, and inclusive communication (Patient Information Forum 2022). This reflects a patient-centred approach, which is highly valued in nursing.
Finally, show that you understand the importance of evaluation. Health promotion is not static. It should be reviewed, improved, and adapted. By including an evaluation plan, you demonstrate accountability and a commitment to evidence-based practice.
By following this guide, and by understanding the why, the what, and the how of health promotion, you can produce a comprehensive and practical assignment. Such work can help you achieve a strong academic result while also preparing you for real-world nursing practice, where promoting health and preventing illness are central parts of the role. Through these assignments, you are developing the skills needed to make every contact count and to support healthier communities in everyday practice (West 2019).
Further reading
To deepen your understanding, it is useful to explore the Ottawa Charter for Health Promotion, as it provides a broader foundation for thinking about empowerment, participation, and supportive environments in public health. It helps place individual interventions within a wider social and policy context.
You may also benefit from reading about motivational interviewing, especially if your assignment involves supporting people who may be ambivalent about change. It complements behaviour change theory by showing how communication style can influence readiness and confidence.
Still struggling with your health promotion assignment? We can help! Our team is qualified and ready to assist with your writing projects. Check out the nursing assignment help page for more info.
References
- Ajzen, I. (1991) ‘The theory of planned behavior’, Organizational Behavior and Human Decision Processes, 50(2), pp. 179–211.
- Michie, S., van Stralen, M.M. and West, R. (2011) ‘The behaviour change wheel: a new method for characterising and designing behaviour change interventions’, Implementation Science, 6, p. 42.
- NHS Digital (2024) Smoking, Drinking and Drug Use among Young People in England, 2023: Key Findings. NHS Digital, Published 17 October 2024.
- Nursing & Midwifery Council (2018) The Code: Professional standards of practice and behaviour for nurses, midwives and nursing associates. London: NMC.
- Patient Information Forum (2022) ‘Reading age guidance for health information’. PIF Position Statement [Online]. Available at: PIFonline.org.uk (Accessed: Day Month Year).
- Phillips, A. (2019) ‘Effective approaches to health promotion in nursing practice’, Nursing Standard, 34(4), pp. 43–50.
- Prochaska, J.O. and DiClemente, C.C. (1983) ‘Stages and processes of self-change of smoking: toward an integrative model of change’, Journal of Consulting and Clinical Psychology, 51(3), pp. 390–395.
- Rosenstock, I.M. (1974) ‘Historical origins of the health belief model’, Health Education Monographs, 2(4), pp. 328–335.
- West, S. (2019) ‘A nurse’s role in promoting health and preventing ill health (from the bedside to the bingo hall)’, NMC Blog, 31 May 2019. Nursing & Midwifery Council.
- World Health Organization (1986) Ottawa Charter for Health Promotion. Geneva: WHO.
Cite This Work
To export a reference to this article please select a referencing stye below:


