Effect of Anticoagulant on Blood Calcium
| ✅ Paper Type: Free Essay | ✅ Subject: Sciences |
| ✅ Wordcount: 1782 words | ✅ Published: 08 Aug 2018 |
Effect of Anticoagulant: Can Heparin Produce Negative Bias in the Determination of Total Blood Calcium?
- Soma Santra1, Manju Soni2, Ajay Soni2, Swati Kotwal1*
KEY WORDS: Quality control, pre-analytical, serum calcium, kit method, o-CPC
Abstract
Calcium is a vital element in the body which plays an important physiological role as it act as a second messenger in many biochemical pathways. Accurate results of total and ionic calcium level plays a pivotal role in patient care and management. Measurement of serum calcium helps to identify many clinical disorders. Many preanalytical conditions affect the blood calcium estimation. The aim of this study is to evaluate the effect of heparin, used as an anticoagulant on total blood calcium assay. Blood specimen from 10 healthy subjects were collected and the difference in total calcium contraction in plasma and serum samples was assessed. No significant changes were observed when plasma levels were compared with the serum values with p value of 0.56. Deming regression analysis yielded the equation: 1.02 × (serum total calcium value) + 0.28 mg/dl. The bias value was -0.109 mg/dl (95% CI: -0.248 – 0.030 mg/dl) for total calcium levels assayed using either tube was acceptable. Total calcium values did not significantly differ when either plasma or serum was used with the spearman correlation coefficients (r value) of 0.98. In conclusion, heparinized tubes can be used for the determination of total blood calcium. The use of plasma sample has an advantage in an emergency laboratory setting due to less processing time.
Keywords: Calcium, Heparin, Quality control, Preanalytical, Phlebotomy, Blood collection device
Introduction
In recent years, there has been an increasing effort by international committees and working groups to develop quality standards for the pre-analytical phase, including the proper use of anticoagulants in sample collection (1, 2). Anticoagulants are additives that inhibit the clotting of blood; they are used only on ensuring that the concentration of the substance to be measured is changed as little as possible before the analytical process (3). The preanalytical laboratory testing takes two major steps: Blood collection and processing (4). The ionic calcium level in blood is recognized to be falsely decreased either due to dilution or binding effects of heparin, which is applied as an anticoagulant (5). The CSLI recommends the use of lyophilized ‘calcium-balanced heparin syringes’ (6, 7) for collecting specimens for ionized calcium measurement. It has been proposed that ionized calcium levels can be affected by excess of heparin present in blood (8), although it was believed that the clinical significance was minimal (9). In this study, we are determining the effect of heparin on assay of total blood calcium to analyze preanalytical error in the collection of blood samples.
Materials and Methods
This study was approved by Swami Vivakanand Medical Mission ethical Committee. Informed consent was obtained from the donors. For evaluation of the effect of heparin on total blood calcium assay, blood samples were obtained from the 10 subjects. Blood samples were sequentially obtained by single venipunture from an antecubital vein in BD PresetR lithium heparin tubes (Ref. No. 367884) and BD vacutainer serum (Ref. No. 367812). All the subjects were between 18 – 50 years age group including both genders. Plasma levels of total calcium were compared to the serum calcium, which was used as a reference here. After the blood withdrawal, samples were then recapped into individual containers, followed by sample centrifugation. The plasma and serum samples were separated within 30 minutes of blood collection. Commercially available biochemical kit (Liquid Gold, Span diagnostic, India) by Arenazo-III method was used for total calcium Assay. Within 2 hours after collection, total calcium was measured in all samples in triplicate and mean was used for further analysis. Data were evaluated using Analyse-it software (version 2.26). For all statistical comparisons, p values less than 0.05 were considered significant. Data concordance was evaluated via Deming regression analysis. The mean of differences (bias) and limits of agreement was calculated using the Bland and Altman method (10). Differences between total calcium level obtained from plasma and serum were compared using the paired t-test. Correlations were determined via calculation of Spearman correlation coefficients (r values).
Results
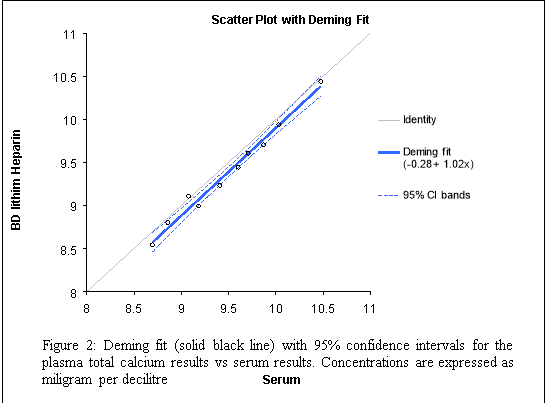
The total calcium values of samples analyzed in the present study ranged from 8.69 – 10.47 mg/dl and the mean total calcium values obtained using BD lithium Heparin was 9.34 ± 0.18 mg/dl whereas that for serum samples was 9.48 ± 0.18 mg/dl with SD of ≤0.57 (Table 1) by 1-way ANOVA. The Spearman correlation coefficient was r = 0.98 (p < 0.0001) when serum and plasma total calcium values were compared. This shows a very good correlation between both samples for total calcium assay (Figures 1 and 2). The bias value was -0.109 mg/dl (95% CI: -0.248 – 0.030 mg/dl) when total calcium of plasma was compared with serum samples (Figure 2). Deming regression analysis of total calcium measurements on samples from all 10 subjects (Figure 2), yielded the following data: slope, 1.02 [95% confidence interval (95% CI), 0.91–1.13]; and intercept 0.28 mg/dl (95% CI, -1.33 – 0.78 mg/dl). The BD Lithium Heparin value was 1.02 × (serum total calcium value) + 0.28 mg/dl.
|
Table 1: Observations on the Effect of Heparin on Serum Total Blood Calcium Estimation. |
||
|
No. of Samples |
BD Vacutainer Serum (mg/dl) (n = 10) |
BD PresetR Lithium Heaprin Tubes, (mg/dl) (n = 10) |
|
1 |
10.48 |
10.44 |
|
2 |
9.08 |
9.11 |
|
3 |
9.18 |
8.99 |
|
4 |
9.60 |
9.44 |
|
5 |
8.86 |
8.80 |
|
6 |
9.71 |
9.61 |
|
7 |
10.03 |
9.94 |
|
8 |
9.41 |
9.23 |
|
9 |
8.69 |
8.54 |
|
10 |
9.87 |
9.70 |
|
Mean ± SE |
9.48 ± 0.18 |
9.34 ± 0.18NS |
|
SD |
0.57 |
0.56 |
|
n = number of subjects; NS: Non-significant; Significant value (p) = 0.56; Difference between samples were evaluated by 1- way ANOVA (p). |

Discussion
Serum is the preferred sample which is used by many laboratories for biochemical testing since it avoids the addition of anticoagulants that may interfere with some analytical methods or alter the true concentration of the parameters being measured. The use of serum or plasma in clinical pathology remains controversial. However, analyte stability is greater in serum
than in plasma (11, 12) and differences between plasma and serum test results have often been documented (13). Moreover, in stored samples, the formation of fibrin strands is lower in serum than in plasma and therefore, there is lesser risk of occlusion in automated biochemical analyzers. However the use of plasma is preferred in some centres as it separates quickly saving preanalytical time thus reducing the total testing period (TTP); secondly, 15–20% more plasma sample can be obtained from the same volume of blood than the serum sample and lastly, with plasma there are no coagulation-induced changes or interferences (3). Heparin has been generally recommended as the most suitable anticoagulant for plasma collection (14) due to its physiological acceptance in vivo. Although in previous reports, a significant differences in selected parameters have been found between heparinized plasma and serum samples (13, 15).
In our study, serum and heparinized plasma yielded similar results with no significant changes in total blood calcium assay this confirms the views of Thorensen, S.I.,et al (15) who also reported similar observations; and this adds up to the observation of Ladenson, J., et al (13) in which clinically significant changes were observed in ionic calcium observations on use of heparinized plasma over serum results.. We found that the Spearman correlation coefficient was 0.98, indicating a good correlation, when total calcium test results when plasma and serum were compared. Deming regression analysis yielded the slope of the regression line that did not approximate unity, suggesting that, in addition to the presence of a small constant bias, a small and non-significant proportional difference also existed between the test results obtained upon use of the two tube types (16). The total calcium assay bias was -0.109 mg/dl. The criteria of acceptable limits imprecision for total calcium assay is 1mg/dl and medically allowable error is 0.37 mg/dl (17, 18). In the present study, we observed that the total calcium concentrations of plasma samples were slightly lower than serum samples with no clinically significant differnece and the bias values were smaller than US CLIA 1988 targets.
Although collection of blood samples from the patients administered with heparin prior to the collection may hold in excess of heparin, increasing clotting time in the collection tube and thereby increasing the potential for the establishment of latent fibrin in the preanalytical phase. Preanalytical variables associated with blood collection should be further standardized to ensure the accuracy of test results. It is impractical to expect tube manufacturers to test out their subway systems on all possible assay platforms; this is a project for individual research laboratories.
Conclusion
We conclude that heparinized tubes are suitable for sample collection for total calcium assay. With the use of heparin tubes use faster processing of blood samples can be possible, which is valuable in an emergency setting and in intensive care units. Moreover, single sample can be used for multiple purpose, including both hematological and biochemical analyses.
References
- Guder, W.G., Ehret, W., da Fonseca-Wollheim, F., Heil, W., Muller Plate, O., Topfer, G. Serum, plasma or whole blood? Which anticoagulant to use? Laboratory Medicine 22, 1998: 297–312.
- World Health Organization. Use of Anticoagulants in Diagnostic Laboratory Investigations. vol. 1 WHO/DIL/LAB/99, Geneva, 1999: 1–64.
- Guder, W.G. The quality of diagnostic samples. Blood Gas News 10, 2001: 18–24.
- Raffick A.R. Bowen, Glen L. Hortin, Gyorgy Csako, Oscar H. Otañez, Alan T. Remaley. Impact of blood collection devices on clinical chemistry assays. Clinical Biochemistry 43, 2010, 4–25.
- Sachs C, Rabouine P, Chaneac M, Kindermans C, Dechaux M. In vitro evaluation of a heparinized blood sampler for ionized calcium measurement. Ann Clin Biochem. 199; 28:240–244.
- National Committee for Clinical Laboratory Standards. Ionized calcium determinations: precollection variables, specimen choice, collection, and handling; proposed guideline. Villonova, PA: NCCLS; 2001. NCCLS Document C31-A.
- Cheung Soo Shin, Chul Ho Chand, Jeong Ho Kim. Liquid Heparin Anticoagulant Produces More Negative Bias in the determination of Ionized Magnesium than Ionized Calcium. Yonsei Med J., 2006; Apr: 47(2):191–195.
- Ritter C, Ghahramani M, Marsoner HJ. More on the measurement of ionized magnesium in whole blood. Scand J Clin Lab Invest Suppl. 1996;224:275–280.
- Toffaletti JG, Wildermann RF. The effects of heparin anticoagulants and fill volume in blood gas syringes on ionized calcium and magnesium measurements. Clin Chim Acta. 2001;304:147–151.
- Bland JM, Altman DG:Statistical methods for assessing agreement between two methods of clinical measurement.Lancet, 1986,1:307–310.
- Boyanton B.L. Jr, Blick KE: Stability studies of twenty-four analytes in human plasma and serum. Clin Chem2002,48:2242–2247.
- Narayanan S:The preanalytic phase an important component of laboratory medicine. Am J Clin. Pathol2000,113:429–452.
- Ladenson, J., Lii-Mei, B., Michael, M.D., Kessler, G., Heinz, J. Serum versus heparinized plasma for 18 common chemistry tests. Is serum the appropriate specimen? American Journal of Clinical Pathology 62, 1974: 545–552.
- Burtis, C.A., Ashwood, A.R., 2008. Tietz Fundamentals of Clinical Chemistry, Sixth ed. WB Saunders, Philadephia, pp. 31–43, 42-62.
- Thorensen, S.I., Havre, G.N., Morberg, H., Mowinckel, P. Effects of storage time on chemistry results from canine whole blood, heparinized whole blood, serum and heparinized plasma. Veterinary Clinical Pathology 21, 1992: 88–94.
- Martin RF: General deming regression for estimating systematic bias and ıts confidenceınterval in method-comparison studies.Clin Chem2000, 46:100–104.
- US Dept. Of Health and Human Services. Medicare, Medicaid, and CLIA Programs: regulations implementing the Clinical Laboratory Improvement Amendments of 1988 (CLIA). Final rule. Fed Regist 1992;57:7002-186.
- Desirable specifications for total error, imprecision, and bias, derived from intra- and inter-individual biologic variation. http://www.westgard. com/biodatabase1.htm.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal