Theories of Fatigue: Football Case Study
| ✅ Paper Type: Free Essay | ✅ Subject: Physiology |
| ✅ Wordcount: 1696 words | ✅ Published: 11 Sep 2017 |
What are the key theories of fatigue, how does it develop throughout the course of a game in footballers and what are its implications on injury risk?
Introduction
Everyone experiences fatigue, and many of us have felt fatigue associated feelings of tiredness, lethargy and slowed reactions it in the context of sport and exercise. Fatigue represents a key limiting factor for performance in sportspeople, and it is therefore a very important topic in Sports Medicine. With this essay, I hope to provide an interesting introduction to the field of fatigue and to demonstrate its importance in sport. The physiological processes underlying the development of fatigue are complex and still widely debated. Nevertheless, I aim to discuss some key theories of the contributing central and peripheral mechanisms, their merits, and how they have developed over time. I will describe how fatigue effects footballers as a match progresses and in doing this, introduce some methods used to monitor the activity of footballers during a game and perhaps prevent injuries. To further highlight the impact of fatigue in sport, I will end by giving evidence that fatigue increases the risk of injury and an important example of how this might occur.
Theories of Central Fatigue
Central Fatigue (CF) describes processes occurring within the Central Nervous System, resulting in a reduced rate of firing by alpha motor neurones to skeletal muscle, and can be summarised as an ‘impaired motor drive’.1 Strong evidence suggests that central mechanisms play a greater role than peripheral mechanisms in fatigue caused by low-intensity exercise.2,3,4 A study published in 20072 illustrates the reduced motor drive caused by CF in low-intensity exercise particularly well. Despite having a relatively low participation of 18, I think it is worth highlighting as it exhibited tight control of unwanted variables. Low-intensity contractions were performed at 20% of maximum voluntary contraction (MVC) and high-intensity contractions at 80% of MVC. Participants were randomised between these two groups and required to perform their respective fatiguing task until failure, which unsurprisingly took longer for low-intensity contractions. Precautions were taken to isolate the elbow flexors including strapping of the shoulder, and neither the subjects nor investigators were informed of their time to task failure as it occurred. Voluntary activation – the increase in force when an electrical stimulus is delivered to a muscle during an MVC – was measured before and after each task. Voluntary activation gives an indication of neural drive and was reduced after both tasks, indicating that CF had affected the elbow flexors. However, the reduction in VA was greater after low-force contractions (14%), suggesting a more significant CF impact than after high-force contractions (5%). In addition, the authors used Electromyography to measure levels of electrical activity in the elbow flexor muscles during and after each fatiguing task. Levels of electrical activity were increased, but measured less after the low-force task, again supporting the theory that CF is primarily responsible for task failure during lower intensity exercise.
A key first hypothesis of the mechanism behind CF, the ‘Serotonin-Hypothesis’, was outlined in a 1987 paper.5 The authors predicted that during exercise, supra-physiological levels of serotonergic activity in the brain were the cause of lethargy and loss of drive during prolonged exercise. This link has been investigated, and it has been shown in rats that a reduced run-time to exhaustion is observed when a general Serotonin antagonist (Quipazine Dimaleate) is administered.6 This effect was not replicated when a Serotonin antagonist restricted to the periphery (Xylamidine Tosylate) was administered. This finding adds weight to the theory that serotonergic activity in the brain, and not in the periphery, plays a role in CF. The mechanism by which exercise causes increased levels of Serotonin is thought to be due to influences it has on the uptake process of Serotonin precursor, Tryptophan, across the blood-brain barrier (BBB).1 More recently, evidence has emerged through studies of amphetamine use 7,8 that dopamine also plays an important role in CF. For example, two papers have shown that a low dose of amphetamine increases endurance in fatigued rats, with endurance being assessed by measuring swimming time and treadmill time to exhaustion.7,8 The mechanism for Dopamine’s role in CF is not completely clear, but its involvement in motivation and reward could be significant.1 The modern theory of CF incorporates all of the above findings, suggesting that an exercise-induced increase in the ratio of Serotonin to Dopamine in the brain is responsible for feelings of lethargy during prolonged exercise.9 If correct, this means that there is the potential to artificially manipulate brain neurotransmitter levels, postpone the onset of CF and boost levels of performance.
Unsurprisingly, given the potential benefits to sports medicine, a lot of research has been done investigating whether the impact of CF in exercise can be reduced. Management of nutrition can be used to artificially manipulate neurotransmitter levels. A number of studies have investigated the administration of branched-chain amino acids (BCAA), which compete with Serotonin precursor Tryptophan for transport across the BBB, on prolonged exercise performance. One such study investigated whether administering a mixture of BCAA to participants during a 30km or 42.2km race could improve race times.10 Unfortunately, the study’s field-based nature meant there was a lack of control over participants during the race. Nevertheless, the authors found that running performance was significantly improved in marathon runners (42.2km) who normally ran at a slower pace, completing the race in 3.05-3.30 hours. Runners who normally posted a ‘faster’ time of under 3.05h showed no significant improvement, leading to the authors’ suggestion that these runners had developed resistance to feelings of CF. This is a fascinating proposition which, if its mechanism can be understood properly, could lead to targeted fitness training for professional sportspeople to overcome the effects of CF. I haven’t been able to find any papers investigating this and believe it would be an interesting topic for future research. As well as managing nutrition, pharmacological manipulation of neurotransmitter levels has been attempted using Serotonin reuptake inhibitors11 and Serotonin Receptor antagonists.12 These papers, along with those investigating nutritional management, struggle to provide a clear consensus regarding the mechanism of Central Fatigue and more robust studies are needed before we can state beyond doubt the roles of Serotonin and Dopamine.
Theories of Peripheral Fatigue
Peripheral Fatigue (PF) describes processes taking place within a muscle, which reduce its capacity to exert force. It is considered responsible for task failure in high-intensity exercise,13 including most exercises performed to build strength. In exercise with high-energy demands on a muscle, anaerobic glycolysis occurs producing lactate. Rates of lactate synthesis outstrip its rate of conversion back to glucose, causing lactate build-up and a shift in equilibrium favouring lactic acid production. Many factors have been suggested as responsible for PF, with early theories citing lactic acidosis as the probable cause,14 although scepticism surrounding this link has since emerged.15,16 A good example of this scepticism is a study which used the ‘Yo-yo intermittent recovery test’ to observe changes in muscle lactate levels and PH, along with other physiological responses, when exercising to exhaustion.16 Participants were asked to run 20m back and forth at progressively increased speeds, until fatigue caused them to twice fall short of the finishing line. Those who had muscle biopsies were sampled on two occasions. During a first run, all 13 were biopsied after exhaustion, with 7 participants also being biopsied at rest beforehand. During a second run on a different occasion, the remaining 6 participants were biopsied at what was calculated to be 90% of their time to exhaustion. The aim of this comparative measure was to observe any change in metabolite levels in the time between 90% and 100% exhaustion. As expected, muscle lactate levels increased eightfold after exhaustion (51.2 ± 7.6 mmol·kg-1) compared to rest (6.8 ± 1.1 mmol·kg-1), and the muscle was more acidic at exhaustion (PH: 6.98 ± 0.04) than at rest (PH: 7.16 ± 0.03). However, there was no observed change in either measurement between 90% and 100% of exhaustion. It should be noted that the samples of only 7 participants were measured for this comparison and a larger participation would have produced even more reliable results. Nevertheless, it is hard to ignore the number of other studies with similar findings15,17 and accordingly, lactic acidosis is no longer considered a determining factor for developing PF. That is not to say that it doesn’t play a smaller role in PF, in combination with other mechanisms. For example, some evidence suggests that acidosis reduces myofibrillar sensitivity to Ca2+ as H+ ions also compete for binding with Troponin C.18
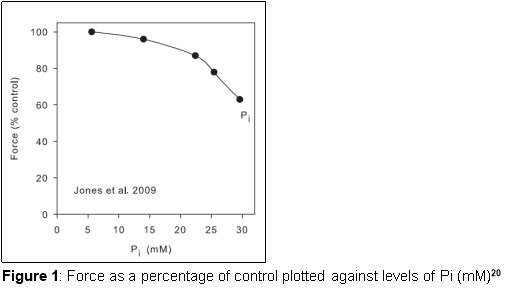
A more popular theory is that Inorganic Phosphate levels are a determining factor for PF. During skeletal muscle activity, Creatine Phosphate (CP) is broken down as part of a process generating ATP, leading to reduced concentrations in exercising muscle. A review of the relevant literature estimated that intense periods of exercise during football matches causes levels of CP to fall by 40%.19 This estimate came after considering the time delay between exercise and biopsy in which resynthesis of CP will take place. Dephosphorylation of CP unsurprisingly leads to increased levels of inorganic Phosphate (Pi) in muscle cells, and this has been shown to correlate with fatigue. One study electrically stimulated the human Tibialis Anterior muscle to induce fatigue and investigate how levels of metabolites changed in relation to reduced contractile force.20 A pneumatic cuff was used to keep the muscle ischaemic, based on the assumption that this would prevent metabolite levels changing between contractions and measuring of metabolites using Magnetic Resonance Spectroscopy (MRS). Metabolites were measured at rest and after 3, 10, 15 and 20 induced contractions. The authors found that force declined to 63% of initial force after 20 contractions. Levels of Pi increased just over fivefold after 20 contractions (29.6 m.moles per litre of intracellular water) compared to at rest (5.6 mmoles) and Figure 1 demonstrates the correlation observed between Pi concentration and Force. Another study used genetically modified mice lacking Creatine Kinase (CK), which catalyses the reaction responsible for regenerating CP, in their skeletal muscle.21 This provided a good model for further investigating the association between Pi and fatigue. Skeletal muscle fibres from the genetically modified mice had a higher Pi concentration at rest compared to wild-type fibres and generated a significantly lower force upon electrical stimulation of tetanus. Additionally, they displayed no significant reduction in force even after 100 induced tetanic contractions, whereas force was reduced to <30% of its initial levels in wild-type fibres. Both findings strongly suggest that increased Pi plays a key role in PF. Further to this, it has been shown that high Pi concentrations in muscle fibres reduces free Ca2+ in the Sarcoplasmic Reticulum,22 meaning less Ca2+ is available for release during force production. The two suggested mechanisms for this are that either high levels of Pi inhibit uptake of Ca2+ by the SR,23 or that Pi enters the SR and precipitates with Ca2+.24
How fatigue develops over the course of a game in footballers
A couple of techniques are used to collect data on footballers’ activity patterns throughout a match. GPS and accelerometer technology can be worn by players during matches to collect data on their locomotor activities.25 Alternatively, it is possible to analyse film of players and use computerised coding to discern their activity patterns to a high degree of accuracy and reproducibility.26 A 2003 study adopting this technique filmed eighteen top-level professional footballers over 129 matches, along with 24 footballers of a moderate standard.27 The authors recorded the frequency and duration of various levels of activity, which were categorised according to speed, and presented the data for every 5, 15, 45 and 90 minutes. This allowed them to compare different stages of the match and pinpoint when levels of athletic performance changed. As well as this, lots of comparisons were made between players of different standards and playing positions which, whilst interesting, aren’t wholly relevant to the topic of fatigue. Top-level footballers ran for longer periods at both low and high intensities, and covered more distance in the first half (5.51 ± 0.10km) compared to the second half (5.35 ± 0.09km) of matches. Figure 2 gives a good visualisation of how distances covered during high-intensity running were unevenly distributed between halves. Distance covered whilst sprinting for top-level footballers was 43% less in the last 15 minutes than the first 15 minutes. Arguably, this could be put down to the fact that the outcome of matches had already been decided as the last 15 minutes approached. However, this is unlikely to be the case because the majority of matches observed had a score difference of only one goal or less approaching this stage, meaning neither team could afford to deliberately lower their intensity. It was also found that substitutes, in comparison to those playing the entire match, undertook 25% more high-intensity running and 63% more sprinting during the last 15 minutes, presumable because they were not fatigued. A 2016 study which used GPS and accelerometer data, presented findings similar to the 2003 study when they observed a significant decrease in locomotor efficiency towards the end of each half in English Championship U21 footballers.25For this study, investigators used a new unit called ‘PlayerLoadâ„¢ per meter’, suggesting that it gives a good representation of locomotor efficiency and may, therefore, be useful for informing decision making before or within a match. For example, squad rotation or training regime decisions could be made base on the locomotor efficiency shown by a player during training or a previous game. This is an example of a very important area of Sports Medicine which is the prevention of injuries by properly managing players outside of match-play. Overall, we can clearly see that footballers become fatigued throughout the course of a match, which I’d like to suggest may be due to the gradual onset of CF. The authors of the 2003 study also wanted to establish whether a ‘temporary fatigue’ effect existed.27 To do this, they identified 5 minutes over which each player covered their peak distance in high-intensity running, representing their most taxing period of exercise for each match. In the 5 minutes following this, on average, each player performed 12% less high-intensity running that the average for all 5 minute periods. This demonstrates that players are affected by a ‘temporary fatigue’ within matches, potentially 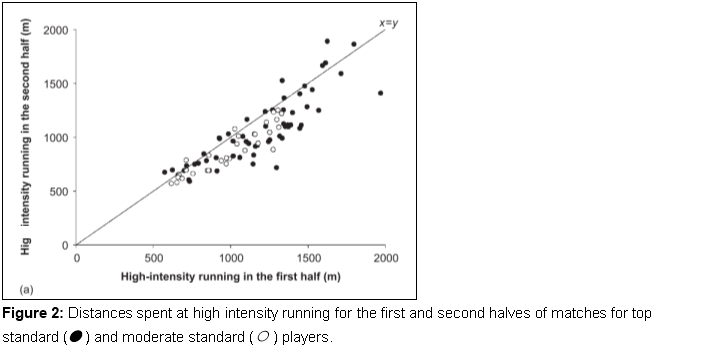 because they are experiencing PF induced by a period of very high-intensity exercise.
because they are experiencing PF induced by a period of very high-intensity exercise.
The implications fatigue on injury risk
Injuries represent a huge challenge for professional sports clubs, as players are rendered unavailable for selection whilst also costing money in wages. This problem is well illustrated by the fact that over 15 seasons for 50 elite football clubs, the average proportion of a squad available for match selection has consistently been below 90%.28 A number of huge epidemiological studies have been set up to investigated the incidence and nature of injuries in professional footballers, 28,29 the most prominent being the ‘UEFA Elite Club Injury Study’ which is updated every season. Over the 2015/16 season, injury data from 29 clubs comprising of an average of 59 matches and 218 training sessions per team was analysed. Over this period, the study found that that on average 0.6 matches and 2.1 training sessions were missed per player per month due to injury.
Data from the ‘UEFA Elite Club Injury Study’ can be used to analyse patterns of injury occurrence during matches. There is an increasing incidence of injuries occurring over time in both halves of football matches, a trend observed in the three most common injury types: strains, sprains, and contusions.28 This strongly correlates with the pattern by which fatigue has been shown to develop over the course of a game,25.27 and it is fair to say that fatigue almost definitely the cause of this increased incidence. A more specific example of how fatigue impacts injury risk can be seen in a 2009 study, set out to establish a link between fatiguing mechanisms and an increased risk of injury to the Anterior Cruciate Ligament (ACL) of the knee.30 ACL injury is particularly devastating for a footballer, not least because of its long-term impacts. A follow up of 176 top level footballers in Sweden who had suffered ACL injuries, found that only 30% were still playing after three years compared to 80% in a control group.31Participation in the 2009 study30 was by 20 female student-athletes who had no history of previous injury to the knee or lower extremities. The biomechanics of participants’ lower limb joints were recorded as they performed randomly ordered, unanticipated jump landings, according to a light stimulus activated just after take-off. They then underwent a fatiguing task consisting of three single leg squats, after which biomechanics were recorded again. This cycle was continued until participants could no longer perform the three single leg squats unassisted, indicating maximal fatigue. Fatigue elicited a number of changes to biomechanics, importantly including a reduction in knee flexion and an increase in the angle of knee rotation, which promote the risk of ACL injury.
Conclusion
The importance Serotonin and Dopamine in controlling CF onset has emerged over time. A developed theory of CF is yet to be proven beyond doubt, despite there being lots of research investigating it. This could be because it is difficult, especially in humans, to structure a study with tight control over the levels of multiple neurotransmitters in the brain. It is also possible that there are more factors contributing to CF which are yet to be identified or supported by evidence. It has been suggested that resistance to CF can be developed through training, which could prove useful to Sports Medicine if investigate further. An early theory involving the build-up of lactic acid in muscle playing a key role in PF has been widely rejected by the scientific, but there is lots of evidence pointing towards increased levels of Pi being a determining factor. Ultimately, PF is probably a combined response to a number of intramuscular mechanisms. Some more potential contributors to this which I have not had a chance to touch upon include depleted glycogen levels in muscle32and altered muscle fibre membrane potentials.33 The influence that fatigue has on sporting performance is significant and can be clearly observed over the course of football matches. Tools exist, including measures of a player’s locomotor efficiency, which play an important role in preventing injury due to fatigue. Whilst there is evidence that fatigue has an impact on cognitive abilities,34,35 there are no studies I am aware of which investigate this in a footballing or sporting context. It would be interesting to see if there is a relationship between fatigue and the quality of a player’s decision making. Epidemiological studies have shown that there is a clear correlation between the onset of fatigue in football matches and a spike in incidences of injuries. There are many examples of injuries for which fatigue is a significant risk factor, with one example being ACL damage. This essay should provide a useful introduction to different areas of interest involving fatigue, all of which can be researched further.
References
- Meeusen R, Watson P, Hasegawa H, Roelands B, Piacentini M. Central Fatigue: The Serotonin Hypothesis and beyond. Sports Medicine. 2006;36(10):881-909.
- Yoon T, Schlinder Delap B, Griffith E, Hunter S. Mechanisms of fatigue differ after low- and high-force fatiguing contractions in men and women. Muscle & Nerve. 2007;36(4):515-524.
- Gauche E, Couturier A, Lepers R, Michaut A, Rabita G, Hausswirth C. Neuromuscular fatigue following high versus low-intensity eccentric exercise of biceps brachii muscle. Journal of Electromyography and Kinesiology. 2009;19(6):481-486.
- ZajÄ…c A, Chalimoniuk M, GoÅ‚aÅ› A, Lngfort J, Maszczyk A. Central and Peripheral Fatigue During Resistance Exercise – A Critical Review. Journal of Human Kinetics. 2015;49(1):159-69.
- Newsholme EA, Acworth I, Blomstrand E. Amino acids, brain neurotransmitters and a function link between muscle and brain that is important in sustained exercise. Advances in Myochemistry. 1987:127-33.
- Bailey S, Davis J, Ahlborn E. Serotonergic Agonists and Antagonists Affect Endurance Performance in the Rat. International Journal of Sports Medicine. 1993;14(06):330-333.
- Bhagat B, Wheeler N. Effect of amphetamine on the swimming endurance of rats. Neuropharmacology. 1973;12(7):711-713.
- Gerald M. Effects of (+)-amphetamine on the treadmill endurance performance of rats. Neuropharmacology. 1978;17(9):703-704.
- Davis J, Bailey S. Possible mechanisms of central nervous system fatigue during exercise.. 1997;29(1):45-57.
- Blomstrand E, Hassman P, Ekblom B, Newsholme E. Administration of branched-chain amino acids during sustained exercise — effects on performance and on plasma concentration of some amino acids. European Journal of Applied Physiology and Occupational Physiology. 1991;63(2):83-88.
- Wilson W, Maughan R. Evidence for a possible role of 5-hydroxytryptamine in the genesis of fatigue in man: administration of paroxetine, a 5-HT re-uptake inhibitor, reduces the capacity to perform prolonged exercise. Experimental Physiology. 1992;77(6):921-924.
- Pannier J, Bouckaert J, Lefebvre R. The antiserotonin agent pizotifen does not increase endurance performance in humans. European Journal of Applied Physiology and Occupational Physiology. 1995;72(1-2):175-178.
- Froyd C, Millet G, Noakes T. The development of peripheral fatigue and short-term recovery during self-paced high-intensity exercise. The Journal of Physiology. 2013;591(5):1339-1346.
- Allen DG, Westerblad H, Lännergren J. The role of intracellular acidosis in muscle fatigue. Adv Exp Med Biol. 1995;384(1):57-68.
- Bangsbo J, Juel C. Counterpoint: lactic acid accumulation is a disadvantage during muscle activity. J Appl Physiol. 2006;100(4):1412-1413.
- Krustrup P, Mohr M, Amstrup T, Rysgaard T, Johansen J, Steensberg A et al. The Yo-Yo Intermittent Recovery Test: Physiological Response, Reliability, and Validity. Medicine & Science in Sports & Exercise. 2003;35(4):697-705.
- Bangsbo J, Graham T, Kiens B, Saltin B. Elevated muscle glycogen and anaerobic energy production during exhaustive exercise in man. The Journal of Physiology. 1992;451(1):205-227.
- Shiraishi F, Yamamoto K. The Effect of Partial Removal of Troponin I and C on the Ca2+-Sensitive ATPase Activity of Rabbit Skeletal Myofibrils1. The Journal of Biochemistry. 1994;115(1):171-173.
- Bangsbo J, Iaia F, Krustrup P. Metabolic Response and Fatigue in Soccer. International Journal of Sports Physiology and Performance. 2007;2(2):111-127.
- Jones D, Turner D, McIntyre D, Newham D. Energy turnover in relation to slowing of contractile properties during fatiguing contractions of the human anterior tibialis muscle. The Journal of Physiology. 2009;587(17):4329-4338.
- Dahlstedt A, Katz A, Westerblad H. Role of myoplasmic phosphate in contractile function of skeletal muscle: studies on creatine kinase-deficient mice. The Journal of Physiology. 2001;533(2):379-388.
- Kabbara Allen D. The role of calcium stores in fatigue of isolated single muscle fibres from the cane toad. The Journal of Physiology. 1999;519(1):169-176.
- Characteristics of phosphate-induced Ca(2+) efflux from the SR in mechanically skinned rat skeletal muscle fibers. Am J Physiol Cell Physiol. 2000;278(1):126-135.
- Fryer M, Owen V, Lamb G, Stephenson D. Effects of creatine phosphate and P(i) on Ca2+ movements and tension development in rat skinned skeletal muscle fibres. The Journal of Physiology. 1995;482(1):123-140.
- Barrett S, Midgley A, Reeves M, Joel T, Franklin E, Heyworth R et al. The within-match patterns of locomotor efficiency during professional soccer match play: Implications for injury risk?. Journal of Science and Medicine in Sport. 2016;19(10):810-815.
- Krustrup PBangsbo J. Physiological demands of top-class soccer refereeing in relation to physical capacity: effect of intense intermittent exercise training. Journal of Sports Sciences. 2001;19(11):881-891.
- Mohr M, Krustrup P, Bangsbo J. Match performance of high-standard soccer players with special reference to development of fatigue. Journal of Sports Sciences. 2003;21(7):519-528.
- UEFA – Union of European Football Associations. UEFA Elite Club Injury Study: 2015/16 season report. Nyon, Switzerland: UEFA; 2016.
- Ekstrand J, Hägglund M, Waldén M. Epidemiology of Muscle Injuries in Professional Football (Soccer). The American Journal of Sports Medicine. 2011;39(6):1226-1232.
- Mclean S, Samorezov J. Fatigue-Induced ACL Injury Risk Stems from a Degradation in Central Control. Medicine & Science in Sports & Exercise. 2009;41(8):1662-1673.
- Roos H, Ornell M, Gärdsell P, Lohmander L, Lindstrand A. Soccer after anterior cruciate ligament injury- an incompatible combination? A national survey of incidence and risk factors and a 7-year follow-up of 310 players. Acta Orthopaedica Scandinavica. 1995;66(2):107-112.
- Ørtenblad N, Westerblad H, Nielsen J. Muscle glycogen stores and fatigue. The Journal of Physiology. 2013;591(18):4405-4413.
- Green H. Membrane Excitability, Weakness, and Fatigue. Canadian Journal of Applied Physiology. 2004;29(3):291-307.
- Féry Y, Ferry A, Hofe A, Rieu M. Effect of Physical Exhaustion on Cognitive Functioning. Perceptual and Motor Skills. 1997;84(1):291-298.
- Abd-Elfattah H, Abdelazeim F, Elshennawy S. Physical and cognitive consequences of fatigue: A review. Journal of Advanced Research. 2015;6(3):351-358.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal