Pathophysiology for Occupational Therapists: Multicple Sclerosis
| ✅ Paper Type: Free Essay | ✅ Subject: Physiology |
| ✅ Wordcount: 2427 words | ✅ Published: 18 May 2020 |
Condition Profile for Multiple Sclerosis
|
Definition of condition |
|
|
Multiple Sclerosis (MS) is an autoimmune inflammatory disorder of the central nervous system(CNS) (Torres & Salazar, Bittner, Zozulya, Weidenfeller, Wiendl, Fahkle, 2008) MS is an insidious disease where large, multifocal, demyelinated plagues, oligodendrocyte loss and axonal degeneration occur on the nerve fibres of the CNS. MS occur when the integrity of the blood- rain barriers is compromised permitting the invasion of monocytes and T cells to the brain parenchyma, resulting in health deficits in an individual. Lesion sights may occur at the cerebrum, optic nerve, cerebellum, brain stem and spinal cord.
https://ot-lwwhealthlibrary-com.ezproxy1.acu.edu.au/content.aspx?sectionid=136769195&bookid=1898 The demyelination means degrading of the myelin sheath (an insulating fatty matter that surrounds the neuron). This stops or slows down nerve conduction thus obstructing and preventing messages passed around the body. There are four types of MS.
This refers the unpredictable exacerbations attacks during which new symptoms appear or existing symptoms become more severe. Relapsing- remitting MS can vary in time (days or months) however partial or total remission can occur.
This is the most common form of MS, present in 60% of patient diagnoses. It involves the progressive acquisition of disability later in the course of the disease may occur. This often associated with superimposed relapses, where the symptoms be unpredictable of time or severity.
This refers to the slow onset and steadily worsening symptoms of the disease without distinct attacks. There is an accumulation of deficits and disability which may level off at some point or continue over months or years. There is a correlation with time and severity present in patients- whereby the longer the progression, the intensifying of the symptoms,
Progressive relapsing is rarely seen in diagnosed MS patient. It refers to the gradual progression of disability from the onset of the disease and is accompanied by one or more relapses. |
|
|
Outline primary body/organ system/s involved |
|
|
Central nervous system The central nervous system (CNS) consists of the brain and the spinal cord. The brain contains about 85 billion neurons and the spinal cord contains about 100 million neurons (Cooke., etl). The CNS is an extremely important structure within the body as it is the source of emotions and thoughts, as well as involved in the stimulation of muscles to contract and glands to secrete thereby controlling body movements and regulations operation of internal organs.
The brain can be divided different sections- responsible for different functions.
(https://www.health.qld.gov.au/abios/asp/boccipital
Neurons of the nervous system (including the PNS and CNS) are responsible for receiving signal, integrating incoming signals and communicate signals to target cells. As seen in the figure below, the neurons within the CNS are composed of three essential parts: (1) a cell body, (2) dendrites and (3) and axon figure.
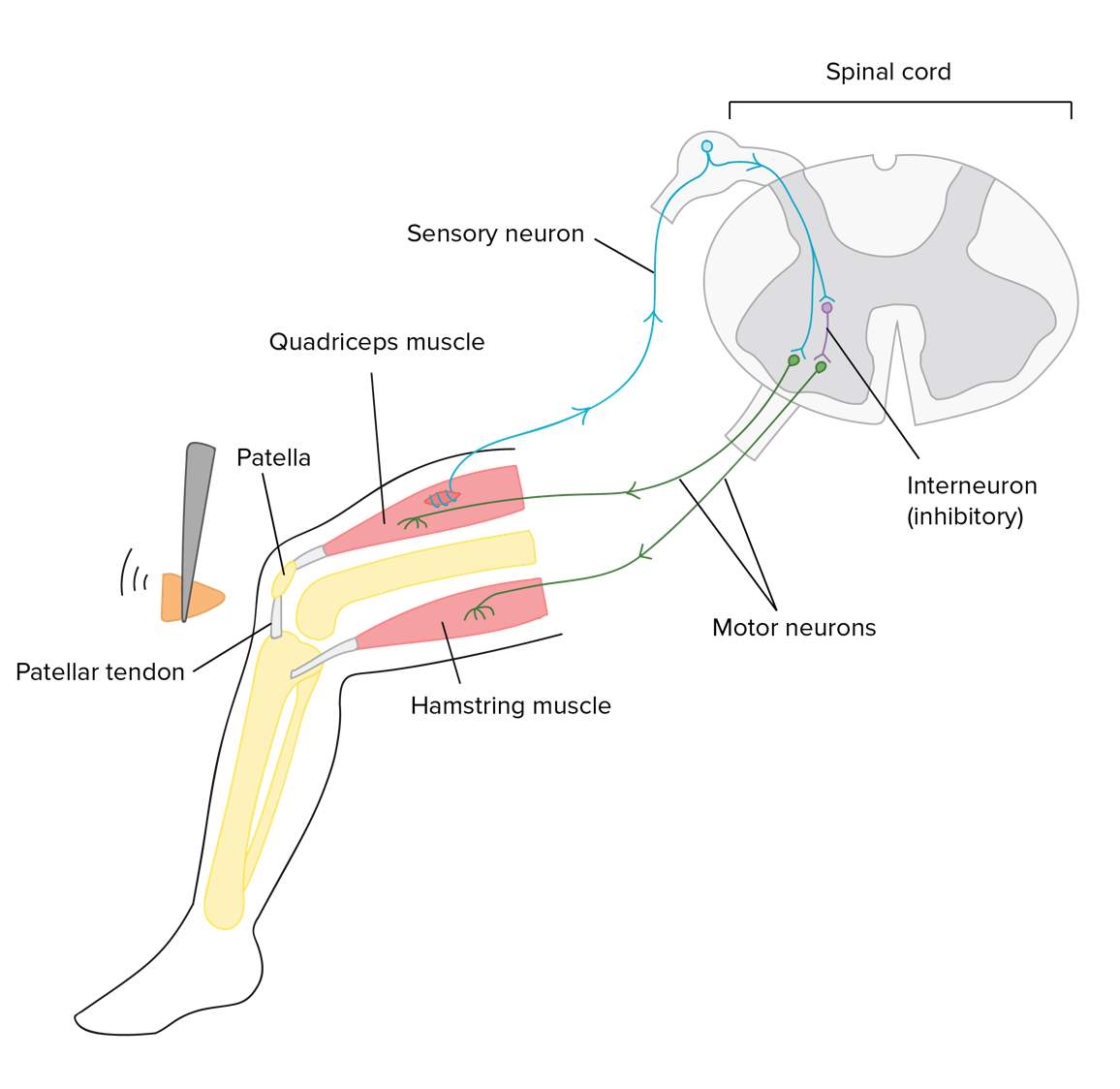
https://www.thoughtco.com/neurons-373486 The brain of the CNS is divided into grey matter and white matter. The grey matter is comprised of the dendrites and the neuron cell bodies, whereas the white matter is comprised of the axon cords that extended to and from neurons. The white appearance is due to the myelin fatty insulating sheath surrounding these axons. This insulating cover allows the nerve consulting signals to travel around the body reliably and quickly. Neurons are electrically excitable. They are able to communicate with each other through electrical impulses (action potential) through short or long distances. For instance, in reflex motions, a potential develops in the sensory receptors of the person skin. This potential activates the axon of the sensory receptor to release an electrical impulse to the interneurons of the CNS. The CNS can then analyse and process this information and causing an electrical impulse to motor neuron thereby allowing the neurons to innervate the muscles of your fingers, causing them to let go.
https://www.khanacademy.org/science/biology/human-biology/neuron-nervous-system/a/overview-of-neuron-structure-and-function |
|
|
Incidence and Prevalence and population affected |
|
|
Worldwide
Australia
https://multiplesclerosis.net/wp-content/uploads/2013/01/global_2x.png |
|
|
Presentation |
|
|
Multiple sclerosis may have a rapid or insidious onset. It is important to consider that every individual is different and may show difference in severity and symptoms. MS affects a wide range of sensory and motors function of the CNS. Symptoms:
Muscle weakness, vertigo (faintness or dizziness) and visual disturbances such as nystagmus, diplopia (double vision) and partial blindness.
Signs: The signs of MS are dependent to the site of lesion in the CNS. An individual presenting MS signs include:
|
|
|
Causes / Aetiology/Risk factors |
|
|
The aetiology of MS is still debatable, but the current data suggests that environmental factors in genetically susceptible background can predispose an individual to M. Clinical study and research there is a genetic (30%) and environmental (70%) influence that may cause the acquisition on MS. (Compston and Coles, 2008) – Studies show a familial recurrence rate of 20% with first aid degree relative (Compston and Coles, 2008) Potential risk factors of MS include infections, vaccination, climate and diet. Infections is considered the most common risk factor for MS due to its molecular mimicry proteins found in the CNS causing activated immune cell attack on CNS. In addition, exposure to viral infections including mononucleosis and the Epstein Barr may have an affect (Compston & Coles, 2008; Wakerley et al., 2012 Other risk factors include latitude, UV light, causation, vitamin D deficiency, obesity, smoking (Hernan, Olek, & Ascherio, 2001) and heavy metal exposure (Noonan et al., 2010) |
|
|
Progression and prognosis |
|
|
The clinical course of MS is variable among individuals, however it usually manifests between 20- 40 years old (Wakerley et al., 2012). Life expectancy of individuals diagnosed with MS has increased, whereby they can expect live seven years less than an individual without the disease (national MDS society) Relapsing- remitting MS This prognosis is usually not severe as it only involves one or two episodes of neurological deficits with no residual impairments. The chance of remaining symptom free increases with each monosymptomatic year. In other words, the more years, the greater the chance of not being impacted by the disease. No immediate or serious intervention is needed, however change in lifestyle is recommended to alleviate any future attacks. Progressive MS The prognosis of an individual with a progressive MS disorder ultimately depends on the severity and worsening of the deficits. Over time, the MS may inhibit many physical functions over the individual which may lead to severe disabling or mortality. Intervention is highly recommended as it may alleviate the prognosis of the individual. Ten years after the disease onset, about 10% will be wheelchair bound and about 50% will be unable to work ([Wakerley et al., 2012]). The median time from disease onset to death is around 30 years ([Compston & Coles, 2008]). |
|
|
Treatment/Intervention: Common medical interventions and management approaches including surgical, pharmacological, lifestyle and psychological |
|
|
Surgical intervention is not part of the routine care given for MS. However, there is strong endorsement towards disease modifying drugs. Drugs such as interferon- B-1b, glatiramer acetate, azathioprine, and fingolimod are particularly useful to help reduce relapses in patients and the progression of MS. ([Carrithers, 2014]; [Harrison, 2014]; [Lyros et al., 2010]; [Wakerley et al., 2012]). Secondary- line disease treatments are useful in promoting antibodies. These include Alemtuzumab and Natalizumab (Carrithers, 2014) In addition, future possible treatment of MS includes transplants of Schwann cells or stem cells and antiviral medication wand vaccination ([Noseworthy, 2003]). Cannabis extract may be used to alleviate pain and in combination with beta blocker to treat spasticity ([Wakerley et al., 2012]). Ant- depressant may be used to treat patient’s affect. Bone marrow transplants are also particularly useful in resetting the immune response and have shown promising effects in reducing relapses In addition, management strategies such as education, healthy diet, no smoking and exercise are particularly low- impact with gradual increase in intensity and frequency can treat fatigue and be useful in alleviating future MS attacks. Donepezil, rivastigmine, and galantamine (initially for Alzheimer’s patients) may improve cognitive symptoms such as attention, information processing, and memory/learning ([Bobholz & Rao, 2003]; [Lyros et al., 2010]). |
|
|
References: |
|
– Exposure to heavy metals within the environment also may play a role (Noonan et al., 2010) – Family history to exposure to viral infections particularly that of mononucleosis and Epstein Barr virus
– Interferon
– Glatiramer acetate – Azathioprine – Fingolmod – Have shown some potential in the reduction of relapse and progression of the disease (Carrithers, 2014;
– Natalizuab – Rituximab – Alemtuzumba – (Carrithers, 2014)
|
|




Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal