Cardiac Anatomy and Function
| ✅ Paper Type: Free Essay | ✅ Subject: Physiology |
| ✅ Wordcount: 2377 words | ✅ Published: 23 Sep 2019 |
The anatomy of the human heart is the same as a lamb’s heart. A heart is a cardiac muscle that works by relaxing and contracting to pump blood around the body by double circulation, where both sides of the heart work to pump deoxygenated and oxygenated blood to the tissues and lungs at the same time for rapid circulation. This allows the blood pressure to remain high by the time the blood reaches the capillaries to improve the efficiency of oxygen distribution, which is essential to sustain the higher metabolic rate in endothermic animals (Toole, 1995). Oxygenated and deoxygenated blood is separated by the septum so the concentrations of oxygen don’t mix. The heart muscle, which is located the thoracic cavity between the lungs protected by the sternum, works involuntary in the way in contracts in a rhythmic sequence as it occurs naturally. As the heart is made up of muscle fibres in the chambers around the wall, they are surrounded by sarcolemma that contains a high number of mitochondria. Mitochondria is a membrane-bound organelle that is the site for respiration to produce energy in the form adenosine triphosphate. This energy used to phosphorylate the cells by converting adenosine triphosphate into adenosine diphosphate for contraction to take place. The pattern of the hear contracting from impulses, makes the heart myogenic. This mean the heart can generate it’s on heartbeat.
A lamb’s heart has four chambers that work together to pump blood to the lungs, kidney, liver and muscles around the body. Both the left and right side of the heart contains an atrium and ventricle, with the left ventricle’s muscle being the thickest to have the ability to pump blood to the rest of the body through the aorta. This process is called ventricular systole where the ventricles contract (while atriums are relaxed) causing the aortic semi-lunar valves to open from the increased in pressure in the ventricles, along with the pulmonary semi-lunar valves. When the pressure in the ventricle, these valves close meaning the ventricles will then be in their relaxed state. Valves prevent the backflow of blood to make sure it only travels in one direction. The atria contracts when the ventricles relax, known as atrial systole and ventricular diastole, blood is the forced into the ventricle when the pressure is high through the bicuspid valve and tricuspid valve.

Figure 1. Anatomy of the heart (OpenStax)
The heart contains different blood vessels that pump deoxygenated blood to the lungs (pulmonary artery) and oxygenated blood (pulmonary vein) to the rest of the body, in which the left side pumps oxygenated blood and the right side pumping deoxygenated. The cardiovascular system is made up of the circulatory system and heart. The mechanism by which oxygenated blood is transported to each cell and removes carbon dioxide and waste products made by cells during respiration. The blood is carried through a complex network of blood vessels called arteries, arterioles, veins, venules and capillaries. They all have different roles and structures in the body, like the veins and venules which deliver deoxygenated blood to the heart therefore their tunica media is thinner than that of an artery, which is made up of smooth muscle cells, elastic tissue and collagen. The capillaries are small vessels where gas exchange takes place and “unite to form venules, eventually flowing into the major systemic veins, the superior vena cava and the inferior vena cava, which return blood to the right atrium” (OpenStax, 2015). Each vessel has a different structure to support its role in the heart and body, this is shown in the figure below (figure 2);
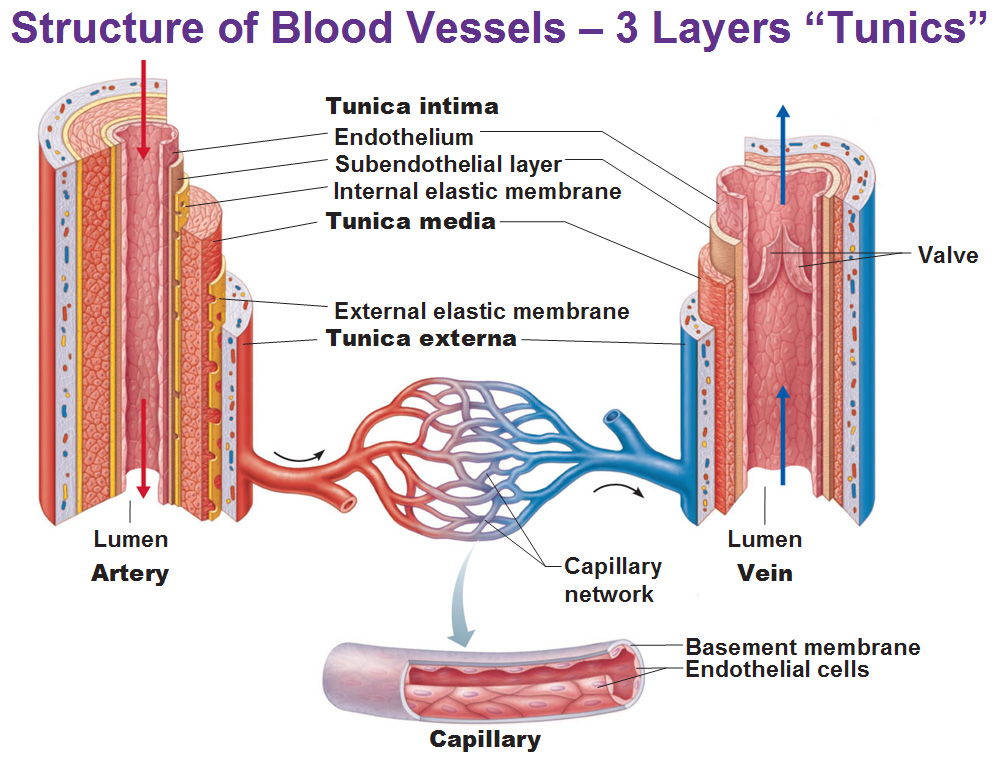
Figure 2. Blood Vessels Structure (Antranik, 2018)
Method and results:
The apparatus used in order to carry out the dissection with health and safety precautions in consideration. Instruments such as a scalpel, dissecting scissors and a tray with protective paper, which had all been sterilized beforehand. Safety equipment used for personal protection included gloves, lab coat and goggles to protect the eyes and skin from any possible irritation. Doing the dissection in a safe, clean and sterile environment was also a safety precaution.
Before the first incision, the heart is placed on the dissection board and analyzed for any damage or if it has any important areas removed, such as the pulmonary trunk that extends off the top of the heart. The left side of the heart must be identified by placing the heart facing up with the auricles covering the top of the atria. Recognizing which side is thicker allows you to know which ventricle, between the left and right, is going to be cut before slicing the heart once the coronary sinus has been found.


Coronary sinus

Auricle
Figure 3. Frontal view of the heart
Figure 3 shows the auricle, which is the flap that covers the atrium. It appears darker than the rest of the heart muscle around it. The pulmonary trunk is located at the front of the heart and enters at an angle.
When the first incision is made from the left side, fingers were used to locate the chambers and different vessels leading from each chamber. This is shown in figure 4 below where a finger had been entered through the left atrium and came out a vessel on the left side of the side of the heart showing that is the pulmonary veins. This is reflected from figure 4 below.

Figure 4. Pulmonary vein
 The second incision on the right side allowed the vena cava and pulmonary artery to be viewed. Shown in the figure below.
The second incision on the right side allowed the vena cava and pulmonary artery to be viewed. Shown in the figure below.
Pulmonary artery

Figure 5. Heart incisions on the left and right side of the heart


Aorta
Bicuspid (atrio-ventricular) valve

Chordae tendinae


Papillary muscle
Figure 6. Detailed examination of the heart
Discussion:
By doing this dissection, it allowed there to be a detailed examination of the heart. Challenges faced in this dissection included the viewing of the pulmonary vein as it had been cut off during the process of removing the heart from the animal. This made it difficult to locate and take a picture of.
The expectations that one would have had before the dissection is that the left ventricle will visibly be thicker than the right. This was proven correct as this could be tested by feeling it by hand before cutting into the heart and also by comparing the thickness after both incisions have been made.
Another challenge was the chambers being larger than expected so finding the valves that lead to a vessel was difficult aswell. This includes the incisions made the cuts may have been deep and splits the valve.
Within my results, some of the images do not show particular vessels, such as the vena cava and the pulmonary artery. This is due to the angles the pictures were taken. This could have been overcome by taking pictures with a hand travelling through the vessel, showing where it is entering and coming out from to get a vivid/realistic view of which one it could be.

Figure 7. Comparison of an athlete and non-athletes heart (David L Prior, 2012)
An athlete’s heart has an increased left ventricular mass and wall thickness. This is known as Athletic Heart Syndrome (AHS), which is common in athletes who routinely exercise for more than an hour a day. Therefore, having this physiological adaptation means the athlete can exercise for a long duration of time. Athlete’s begin to respire anaerobically when they run because their muscle cells use up oxygen quicker than they can remake it. This is beneficial because anaerobic respiration is quicker than aerobic. Figure 1 suggests the whole heart is bigger in athlete’s because the chambers show to be bigger and they have thick ventricular wall. This allows more blood to be pumped into the heart during one beat as the heart rate is slower than a non-athlete. Therefore, more oxygen can be transported to the lungs in a quicker time, compared to a none athlete who’s heart fills blood every few seconds, hence it having a rapid heartbeat.
- Deoxygenated blood flows through the pulmonary artery from the right ventricle to transport the from the heart to the lung. Oxygenated blood is then delivered back to the heart through the pulmonary vein into the left atrium. This is shown in the example figures below.


Figure 8. (Thomas G. 2013)
Figure 9. “Pathway of blood flow through the heart and lungs. (Modified from Tortora and Grabowski, 2000).”
Venous blood leaves the pulmonary trunk after ventricular systole occurs, where the muscle wall of the ventricles contract to force blood out. When this blood leaves the pulmonary vein, the semi-lunar valves close and the lungs receive the blood where it will be converted into arterial blood.
Blood doesn’t have to travel far between the heart and lungs because the hear lies between the right and left lungs, behind the breastbone and is slightly to the left (Natural Remedy Ideas, 2018). This makes the delivery of oxygen quicker and more efficient by the red blood cells.

Vena Cava
Tricuspid Valve




Right lung
Pulmonary Vein

Right Atrium
Left Atrium
Bicuspid Valve

Pulmonary Artery


Left ventricle
Right Ventricle
Semi lunar Valve
Left lung
Aorta
Semi lunar Valve
- The graph to show comparisons between an athlete and sedentary heart is shown below


From the graphs you can identify that person A is a trained athlete because the cardiac output is higher than person B. The cardiac output increases when the heart rate and stroke volume is increased (G. Wooldridge, 2015). The is because the equation to calculate the cardiac output is stroke volume multiplied by heart rate, therefore when either one or both increase, it will increase the cardiac output value. In the athlete’s case, they have a maximal stroke volume which causes their cardiac output to be high even though their resting heart rate is low. By it having a slow heart rate allows more time for ventricular diastole to occur, so that more blood can enter to leave and go to the lungs. This decreases the sympathetic activation that decreases intrinsic sinus node activity that may play a role in electrical activity. Person A’s slow heartbeat results to bradycardia in athletes as it means are not many protein channels to transfer currents that control heart activity. Electrical signals won’t be able to be sent from the sinoatrial node, slowing down impulses across the atrium (Brookshire, 2014). Bradycardia can decrease the myocardial oxygen demand increasing haemoglobin total and blood volume enhances oxygen transport.
Livestrong.com says that a non-athlete hear rate, at its resting state, should be around 60 to 100 beats per minute. Their stroke volume will increase from 70 ml to 120 ml per beat in trained athletes. This immense change is caused by more sympathetic nerves being output to the heart, increasing the release of adrenaline in the blood that, in turn, increasing the stroke volume.
- Hypertrophic cardiomyopathy is where the muscular wall becomes much thicker than the athlete’s heart. This restricts blood from flowing through easily as the walls block the semi-lunar and bicuspid valves slightly putting the person at risk of death. In comparison, the athlete’s heart has a thick wall but not enough to let blood enter but it will provide more energy from the high abundance of mitochondria in the muscle cells to be able to pump blood through the aorta to the rest of the body. The chambers in the athlete’s heart are enlarged so more blood can be collected but on the other hand, with hypertrophic cardiomyopathy, the chambers aren’t large enough to collect enough blood due to the thickness of the walls. The heart wall cells are stacked tightly in stacked straight lines allowing electrical signals to travel through smoothly and quickly. This is different to the muscle wall cell structure of cardiomyopathy because they are larger and more spaced out. They are not arranged in a pattern, making the signals transport slowly. This forces the heart to work harder and makes it tough for it to fill with blood when it relaxes.

Figure 10. Comparison between all three heart types (George Van Der Walt, 2017, https://www.pinterest.co.uk/pin/538883911635172190/ last accessed: 22.11.18)
|
|
Athlete’s Heart |
Hypertrophic Cardiomyopathy |
|
Similarities
|
Both are related to wall thickness Both have an increased heart size as a whole |
|
|
Differences |
This cannot be inherited This syndrome is beneficial to athletes Heart muscle wall cells are tightly packed The chambers are enlarged Heart rate is slow but under less pressure to pump blood in one beat |
This can be inherited and can be a result of a defect in the genes that control the growth of the heart. This can cause death in athletes/people The muscle wall cells are not tightly part so are more spaced out but touch slightly The chambers are more tightly squeezed Heart rate is slower to pump blood efficiently as it is under more stress |
References:
- Antranik. Blood Vessels. Available: https://antranik.org/blood-vessels/. Last accessed 21/11/18
- Bethany Brokshire. (2014). A Slow Hearbeat in Athletes is Not So Funny. Available: https://www.sciencenews.org/blog/scicurious/slow-heartbeat-athletes-not-so-funny. Last accessed 22/11/18.
- C.J. Clegg, D.G. Mackean. (Jun 1994). Chapter?. In: Advanced Biology: Principles and Applications. London: John Murray. pp 01.
- David L Prior, Andre La Gerche. (2012). The Athlete’s Heart. Available: https://heart.bmj.com/content/98/12/947. Last accessed 22
- Glenn and Susan Toole (2015), AQA Biology. 2nd ed. Oxford University Press, pp.170, 171
- John Hurray. (2018). Where is Your Heart Located? Chest Pains Related with Your Heart. Available: https://naturalremedyideas.com/where-is-your-heart-located. Last accessed 22/11/18.
- Karen Hellesvig-Gaskell . (2017). Differences Between Athletes & Nonathletes. Available: https://www.livestrong.com/article/493788-differences-between-athletes-nonathletes/. Last accessed 22/11/18.
- Kjetil Lenes. Heart Anatomy. Available: https://courses.lumenlearning.com/nemcc-ap/chapter/heart-anatomy/. Last accessed 21/11/18.
- Lizzie Brooks. (2018). The Advantages of Anaerobic Respiration. Available: https://sciencing.com/advantages-anaerobic-respiration-6874497.html. Last accessed 22/11/18.
- OpenStax. Heart Anatomy. Available: https://courses.lumenlearning.com/nemcc-ap/chapter/heart-anatomy/. Last accessed 21/11/18
- Paul A. (2017). The Human Heart. Available: http://www.vhlab.umn.edu/atlas/physiology-tutorial/the-human-heart.shtml. Last accessed 22/11/18./11/18.
- Robert S. McKelvie. (2017). Athlete’s Heart. Available: https://www.msdmanuals.com/en-gb/professional/cardiovascular-disorders/sports-and-the-heart/athlete’s-heart#resourcesInArticle. Last accessed 21/11/18.
- Thomas G. Brock (2013). APIs – Prostaglandins with a Purpose. Available: https://www.caymanchem.com/article/2210. Last accessed 21/11/18.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


DMCA / Removal Request
If you are the original writer of this essay and no longer wish to have your work published on UKEssays.com then please click the following link to email our support team:
Request essay removal