Pathways to Resilience in the Context of Somali Culture and Forced Displacement
Info: 48730 words (195 pages) Dissertation
Published: 28th Feb 2022
Tagged: Cultural StudiesPsychology
Abstract
Little is known about resilience among Somali refugees. This study employed a participatory, sequential, mixed-method research design to: a) culturally adapt and validate the Resilience Research Center- Adult Resilience Measure (RRC-ARM) for use with Somali people; and b) Explore pathways to resilience in the context of Somali culture and forced displacement.
The study was completed in three phases. First, interviews were conducted with resilient Somali people (n = 10) living in the US. These interviews produced information about Somali conceptualizations of resilience and informed selection of study measures administered during phase three. Second, study measures were translated and back-translated. Third, a quantitative survey of resilience, life difficulties, well-being, and meaning in life was administered to 137 Somali people living in the US.
An exploratory factor analysis of the RRC-ARM produced a three-factor structure (viz., individual, relational, and cultural) with good internal consistency and convergent validity. Evidence was also found to support the incremental validity of the measure. Resilience positively associated with presence of meaning in life; and meaning in life predicted a good portion of variance in well-being. The qualitative findings suggest that “presence of meaning in life” is reflective of the broader influence of Islam on understanding life experiences in the context of Somali culture; and resilience resides within broader geographic and political contexts that influence access to resources that promote health and well-being. Qualitative and quantitative findings were integrated to develop the Somali Multidimensional and Multilevel Resilience (SMMR) model. Key elements of the model include the factors that emerged from EFA and a hierarchy of health-sustaining resources, all nested in a form of existential resilience experienced through Islam and presence of meaning in life.
The Somali RRC-ARM seems to be a psychometrically sound measure of resilience with Somali people. Complementing administration of the Somali RRC-ARM with qualitative data is essential for proper interpretation of quantitative data. The SMMR Model provides a framework from which to assess resilience factors across multiple dimensions and multiple levels across a variety of contexts and promotes strengths-based programming and practice.
Chapter 1: Introduction
This study employed a participatory, sequential, mixed-method (qualitative-quantitative) research design to explore resilience in the context of Somali culture and forced displacement. The research design ensures that quantitative data reflected the underlying cultural and contextual realities of Somali refugees. Qualitative information provided context to quantitative data. Cultural advisors contributed to research design, methodology, selection of culturally relevant measures of variables that may be theoretically related to resilience, and interpretation of study findings. Researchers and research assistants worked closely with professional consultants, cultural advisors, and community partners to produce the first psychometrically sound measure of resilience for Somali refugees and the Somali Multidimensional and Multilevel Resilience Model. This chapter presents the background and significance of studying resilience in the refugee context is presented, followed by an overview of research design and methodology. The chapter closes with a problem statement and presentation of research questions and study aims.
Background and Significance
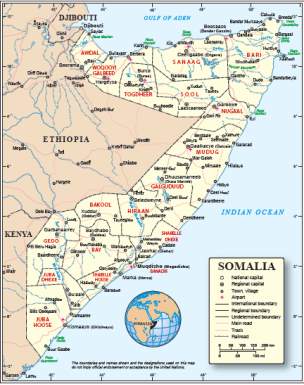
Figure 1: Map of Somalia
Somalia is a country located in the northeastern corner of Africa in a region commonly referred to as the Horn of Africa (Google Maps, 2013). In 1991, local rebel groups overthrew the government of Somalia. Mogadishu and most of southern and central Somalia disintegrated into civil war. Simultaneously, a deadly drought settled over the region (Abdullahi, 2001). With no formal government in place, food and power belonged to those with guns (Putnam & Noor, 1993). Over the course of one year, hundreds of thousands of Somali people died from political violence, disease, and famine. According to the Centers for Disease Control and Prevention (CDC), by August 1992, about one fourth of the population of Somalia was in danger of starvation. At least 40% of the population in the city of Baidoa died between August and November, and various relief organizations estimated that one half of all Somali children under five years old had died (CDC, as cited by Putnam & Noor, 1993). Conflict in Somalia continues today, especially in central and southern regions of the country. According to the United Nations High Commissioner for Refugees (UNHCR; 2010), about 1.4 million people are internally displaced within Somalia and over 600,000 Somali people have taken refuge in Kenya and Ethiopia.
High rates of exposure to adversity among Somali refugees are well documented. The most commonly reported adverse experiences include political violence, death of loved ones, torture, rape, and starvation (Bhui et al., 2003). Conditions in refugee camps are only slightly better than Somalia. Food and water are in short supply, security is minimal, and livelihood opportunities are nearly non-existent in refugee camps (Ingleby, 2005). Many Somali refugees spend years, even decades in refugee camps, waiting for a durable solution to their crisis. Only small fractions of people are considered for resettlement in a third country. Those who are resettled in a third country encounter additional forms of adversity, including acculturation stress and racial discrimination (Young, 2006).
Research suggests Somali refugees experience high rates of physical illnesses (e.g., diabetes, hypertension, chronic pain) and mental health disorders (e.g., depression, anxiety, PTSD) following resettlement (Bentley & Olson, 2008; Halcón et al., 2004; Jaranson et al., 2004; Robertson et al., 2006). According to Bentley and Olson (2008), Somali refugees rarely seek mental health treatment due to social stigma and differences in conception of mental disorder across cultures.
Western culture views mental health from the perspective of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994). According to the DSM-IV, individuals experience a range of thoughts, emotions, memories, and sensory experiences that combine to create general psychological experience. Love, grief, anxiety, sadness, stress, posttraumatic stress, intellectual disorders, and developmental disabilities are dimensions of psychological experience considered within the Western conception of mental health and illness (Arnett, 2012). Seeking mental health services is not uncommon in Western culture and services include a range of approaches from brief psychotherapy to long-term, residential treatment (Pomerantz, 2010).
In comparison, Somali culture views mental health more dichotomously: one is either sane or insane (Bentley & Olson, 2008). The sane may experience many conditions Western culture labels as disordered, such as sleep disturbance, nervousness, fatigue, headache, and sadness. Traditionally, Somali people consider these types of experiences a normal part of life, spiritual challenges to overcome. Mental disorders are highly stigmatized in Somalia. Families often isolate and care for the insane alone, or the individual is hospitalized indefinitely (Bentley & Olson, 2008).
Some researchers have sought to understand barriers to help-seeking behavior among refugee populations in general (Ingleby, 2005), such as communication difficulties and lack of understanding of the healthcare system in the US. Public health initiatives have focused on decreasing stigma associated with mental disorders among diverse populations in an effort to boost help-seeking behavior (Henderson, Evans-Lacko, & Thornicroft, 2013). These efforts rest on at least two assumptions: a) Western mental health services are the best avenue for addressing mental distress among Somali refugees; and b) correcting Somali conceptions of mental disorder will lead to increased engagement in the context of traditional Western mental health services. Given the choice, however, it seems most Somali people prefer to cope with mental health concerns within the family system and through spiritual practice and prayer (Bentley & Olson, 2008).
According to Luthar, Cicchetti, and Becker (2000), “resilience refers to a dynamic process encompassing positive adaptation within the context of significant adversity” (p. 543). The construct offers an alternative lens through which to consider health and well-being. Resilience research began in the early 1980s when researchers first became interested in the subpopulations of peoples who were adapting and developing well despite the experience of adversity. A robust body of literature on resilience has developed since that time, contributing to an understanding of individual and environmental dimensions of the construct (Anthony & Cohler, 1987; Garmenzy, Masten, & Tellegen, 1984; Kobasa, 1979; Luther et al., 2000; Scales & Roehlkepartain, 2003; Werner & Smith, 2001).
This literature has developed, however, with little attention paid to the role of cultural and contextual factors in the understanding, expression, and experience of resilience (Liebenberg & Ungar, 2009). The study of resilience presents an alternative avenue for understanding health and well-being among Somali populations that is focused on strengths as opposed to deficits and disorders. Most quantitative measures of resilience, however, were developed based on Western cultural norms and assumptions. Indeed, out of 15 measures of resilience identified in a literature search of the EBSCO database (see Appendix A), only one measure, the Child and Youth Resilience Measure (CYRM), was developed and validated for use cross-culturally (Ungar & Liebenberg, 2011).
The CYRM was developed by the International Resilience Project (IRP), which is a part of the Resilience Research Center (RRC) located at Dalhousie University in Fairfax, Nova Scotia. Drs. Michael Ungar and Linda Liebenberg are co-directors of the research center and principal investigators on the IRP, a multisite, cross-cultural investigation of resilience among children living in developing nations and children living among marginalized populations within developed nations (Ungar & Liebenberg, 2009).
Using an iterative and participatory model of mixed-method research to investigate resilience, IRP brought together over 40 researchers across 14 research sites in 11 countries. They developed and pilot-tested the innovative CYRM across the 14 research sites, analyzed findings from the administration of the CYRM to 1451 youth globally, collected 89 interviews and life histories from children across sites, conducted 5 focus groups with youth and 12 interviews with adults in different communities, and collected field notes on the process of the study design.
The IRP predicted the CYRM to sort into an ecological model similar to that proposed by Bronfrenbrenner (1979), but the researchers were unable to produce a valid and stable factor structure across all cultures and context. Scores did not sort neatly into the hypothesized model. Qualitative data helped contextualize differences observed across cultures. Ungar (2008) concluded that cultural context shapes how ecological components of resilience (e.g., family, community) contribute to the expression of resilience. Therefore, qualitative and quantitative methods alone cannot capture resilience completely, which suggests mixed-methods are necessary. Indeed, Ungar and Liebenberg (2011) recommend complementing quantitative data with qualitative inquiry and participant input to ensure the validity of data interpretation. The RRC recently adapted the CYRM for use with adult populations (Liebenberg, 2011, personal communication), resulting in the RRC-Adult Resilience Measure (RRC-ARM; Liebenberg, 2012, personal communication).
The present study is theoretically aligned with the work of the RRC and IRP. Following Ungar and Liebenberg’s (2011) recommendations, this study employed a partially participatory, sequential, mixed-method research design to:
- Explore the factor structure, construct validity, and clinical utility of the RRC-ARM when administered to a Somali population;
- Examine pathways to resilience in the context of Somali culture and forced displacement.
The following definition of resilience guided our inquiry:
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways (Ungar, 2008, p. 225).
Research Design and Methodology
This study employed a participatory, mixed-method research design in three phases. During phase one, the research team conducted interviews with resilient Somali people (n = 10) living in the US about experiences of health and well-being in the context of adversity across three distinct contexts (i.e., Somalia, refugee camps, US). These interviews produced information about Somali conceptualizations of resilience and informed selection of study measures (with support of the cultural advisors) to be administered during phase three. During phase two, study measures were translated and back-translated in an iterative process until deemed culturally equivalent by translators and cultural verifiers. During phase three, a quantitative survey of resilience, life difficulties, well-being, and meaning in life was administered to 137 Somali people living in the US. Qualitative and quantitative data were analyzed separately and then integrated to develop a multidimensional model of resilience for Somali refugees.
Cultural advisors
Ungar and Liebenberg (2009) recommended collaborating with cultural advisors and community members when researching resilience. Our research team included three cultural advisors with whom we collaborated on each phase of the study. Cultural advisors were chosen because of their own experience overcoming adversity and their understanding of Somali culture, language, and community, and their interest in the project.
Cultural advisors were involved in:
(1) the conceptualization of the research project;
(2) the development of the key-informant interview protocol;
(3) conducting key-informant interviews;
(4) selecting, translating, and adapting study measures;
(5) consulting on the survey format;
(6) connecting the project with community organizations who helped facilitate quantitative data collection;
(7) general cultural navigation; and
(8) the interpretation and presentation of research findings.
Meetings were held as needed, most typically in the form of telephone conversations, followed by email communications. Many other Somali community members, as well as many academic and professional consultants, were less formally involved in shaping the project.
Problem Statement and Study Aims
Somali people form one of the largest and fastest-growing refugee populations in the world (UNHCR, 2010). Research documents extremely high rates of exposure to adversity among Somali refugees, including political violence, death of loved ones, torture, rape, and starvation (Schuchman & McDonald, 2004). Likewise, many researchers have observed high rates of psychopathology among Somali refugees following resettlement (Halcón et al., 2004 Jaranson et al., 2004; Robertson et al., 2006). Despite high rates of exposure to adversity and high rates of psychopathology (e.g., PTSD, depression), Somali refugees often are reluctant to utilize Western mental health services (Bentley & Olson, 2008). The academic literature disproportionately focuses on pathology, as defined by Western cultural norms and expectations, with little attention paid to resilience among Somali refugees. Resilience may be an alternative avenue toward understanding and promoting well-being among Somali refugees living locally and globally. However, a measure for examining resilience among Somali refugees has not yet been validated, and little is known about how resilience is conceptualized among Somali people.
To begin to address these gaps in the literature, and elucidate pathways to resilience among Somali refugee populations, the present study:
- Qualitatively explored resilience and well-being among Somali refugees using key-informant interviews;
- Identified additional study measures based on qualitative findings and consultation with cultural advisors;
- Translated and back-translated all study measures;
- Administered a survey of resilience, life difficulties, personal well-being, and meaning in life to a purposive sample of Somali people living in the US;
- Produced data on the factor structure and psychometric qualities of the RRC-ARM when administered to a Somali population; and
- Integrated qualitative and quantitative data into a multidimensional model of resilience in the context of Somali culture and forced displacement.
Chapter 2: Literature Review
Global Refugee Crisis
The United Nations High Commissioner for Refugees (UNHCR) documented 43.7 million forcibly displaced persons living worldwide at the close of 2010 (UNHCR, 2010). The organization cited political violence and persecution as the driving force behind displacement. This is the highest reported number of forcibly displaced persons in over 15 years. To aid in comprehension of the following literature review, I will use the term refugee broadly to include all seven UNHCR categorizations of forcibly displaced persons: refugee, asylee, internally displaced person, stateless person, returned refugee, returned internally displaced person, and others of concern. These categories are described here to offer an appreciation for the breadth of experiences encompassed by the global refugee crisis.
Forcibly displaced populations
According to Article 1A of the 1951 United Nations Convention Relating to the Status of Refugees, a refugee is a person who:
Owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group, or political opinion, is outside the country of his nationality, and is unable to or, owning to such fear, is unwilling to avail himself of the protection of that country (UNHCR, 1951, p. 1, as cited by UNHCR, 2012).
An asylee is defined exactly as a refugee in the definition above. Unlike refugees, however, asylum seekers arrive in the host country before they have evaluated the asylum claim. Refugees typically arrive in host countries en masse from known conflict areas. UNHCR grants asylum upon registration at the refugee camp. Asylum seekers must prove they have a well-founded case constituting designation as a refugee before they are granted asylum in the host country. This process results in legal fees, living under the threat of forced repatriation to their country of origin, and at times, indefinite confinement (Ingleby, 2005). Once granted asylum, asylees share similar access to immigration and social services as refugees.
An internally displaced person (IDP) is one who is displaced within the borders of their home country due to war, persecution, or natural disaster. IDPs are officially nationals of their home country, and their home government is officially responsible for their protection. IDPs are often displaced due to government-fueled war or persecution, placing their very protection in the hands of their persecutors. IDPs are particularly vulnerable populations. They are difficult to access due to their dispersion in war torn areas, making aid and other service delivery challenging. Although the number of IDPs is difficult to estimate, UNHCR (2012) reported over 27.5 million IDPs received their assistance in 2010. This is the highest number of IDPs ever recorded; nearly double the figure from 2005 (UNHCR, 2012).
A stateless person is one who lives without formally acknowledged nationality or citizenship in any State. Statelessness occurs for many reasons, including discrimination against minority groups in nationality legislation and failure to include all citizens when states declare independence. Stateless persons live on the fringes of society, often unable to obtain documentation of their identity. Without identification, stateless persons are often detained and denied access to education and health care services. About 12 million stateless people live worldwide (UNHCR, 2010).
Returned refugees and returned IDPs are the populations of people who are able to return to their country of origin to an environment deemed adequately safe by the UNHCR. Only 197,600 refugees were returned to their country of origin in 2010, the lowest number in two decades. This low number is offset by the 2.9 million IDPs returned to their home communities in 2010, the highest number on record in 15 years. Others of concern are a UNHCR category of displaced persons who do not fit one of the previous definitions of forced displacement but still receive aid or benefits from UNHCR programming (UNHCR, 2012).
Durable solutions
After fleeing persecution, many refugees spend years, even decades in refugee camps, waiting for a durable solution to their crisis. The UNHCR outlines three durable solutions for forcibly displaced populations: a) repatriation to their country of origin; b) integration into the local (host) community; or c) resettlement in a third country.
Repatriation has steadily decreased since 2004. As previously noted, only 197,600 refugees were returned to their homes in 2010, the lowest number reported in two decades. Integration into the local (host) community is uncommon due to a constellation of legal, economic, and sociocultural challenges (UNHCR, 2010). Finally, less than 1% of the total refugee population resettles in a third country (Ingleby, 2005).
Resettlement has slowed in recent years due to increased security measures and screening protocols for refugees seeking resettlement (UNHCR, 2010). In 2010, the UNHCR submitted more than 108,000 refugee cases for consideration; 22 countries accepted refugees for resettlement and only 98,800 refugees were resettled. Many refugees find themselves in protracted situations, defined by the UNHCR as:
Situations in which refugees find themselves in a long-standing and intractable state of limbo. Their lives may not be at risk, but their basic rights and essential economic, social and psychological needs remain unfulfilled after years of exile (UNHCR, 2006, p. 106).
One such situation is evident along the borders of Somalia where 70,000 Somali refugees have fled to neighboring countries in the past year alone, contributing to the world’s largest protracted refugee crisis (UNHCR, 2011).
Somali refugees
Somali refugees comprise one of the largest and fastest growing refugee populations in the world (UNHCR, 2011). Following the fall of government in 1991, Somalia has been in a brutal civil war, prompting large numbers of men, women, and children to flee the country seeking refuge in bordering countries (Putnam & Noor, 1993). Many other Somali people remain displaced within Somalia’s borders (UNHCR, 2011).
Due to ongoing political violence and famine, the UNHCR and other humanitarian aid organizations reported a dramatic increase in the number of Somali refugees in recent years (Médicins Sans Frontières, 2009; UNHCR, 2011). Since 2008, over 120,000 Somalis have entered Kenya as refugees, and over 70,000 new Somali refugees have arrived in Dadaab refugee camp in Kenya, making the camp the largest in the world (UNHCR, 2011).
The UNHCR originally established Dadaab to accommodate 90,000 refugees. It is now over three times that capacity, and more than 5,000 refugees continue to arrive at the camp monthly—exhausted, malnourished, and in need of immediate medical attention (Médicins Sans Frontières, 2009). According to the UNHCR (2011), Dadaab represents a protracted refugee situation and one of the most acute emergencies in the world.
Mental health of refugees
Global concern for the mental health of refugees has increased in recent years. Policy makers and healthcare providers are increasingly recognizing mental healthcare as a priority for many refugees (Ingleby, 2005). Many studies document high prevalence of mental health disorders among refugee populations. Refugees experience high rates of mental disorders due to a constellation of pre-migration and post-migration stressors. The body of literature reflects studies conducted with refugee populations since the early 1980s. Researchers in Western academic institutions have conducted most studies on refugee mental health, such as The Harvard Trauma Center, which developed the Harvard Trauma Questionnaire (HTQ) and adapted the Hopkins Symptoms Checklist (HSCL) for use with refugee populations. Researchers consider these measures the gold standard screening measures for PTSD, anxiety, and depression among refugee populations. The HTC and HSCL have demonstrated good reliability across many studies (Bentley, 2011; Jaranson et al., 2004; Mollica et al., 2002).
All of these studies, however, must be understood within the context in which they occurred. Most studies of refugee mental health impose a Western model of disorder without careful consideration of cross-cultural validity. Measurement tools are most often developed by Western researchers and validated among large samples of Western participants. When these tools are translated and administered to non-Western populations, researchers must take caution to ensure the validity of data. Translation and back-translation is an iterative and active process. Researchers seldom explain thoroughly how and why the measure was deemed equivalent in meaning across cultures.
History of refugee mental health research
Early contributions to the refugee mental health literature came during the 1980s when Southeast Asian populations (viz., Cambodian, Vietnamese, and Hmong/Laotian) first resettled in the West. Researchers conducted a longitudinal study of PTSD among a group of Cambodian youths (n = 46) who had endured internment in Khmer Rouge re-education camps (Kinzie, Sack, Angel, Clark, & Rath, 1989; Sacks, Angle, Kinzie, & Rath, 1986). The Pol Pot regime subjected these youths to forced labor, beatings, and starvation. Each lost an average of three family members due to the violence. Four years after departure from Cambodia, over 50% met diagnostic criteria for PTSD (Kinzie et al., 1986). At three-year follow up, the researchers found nearly identical rates of PTSD (Kinzie et al., 1989). Unfortunately, they were unable to determine whether the same youths experienced the disorder, or if there were unique cases.
Mollica and colleagues (1993; 2002) published a group of studies documenting rates and correlates of PTSD and depression among Southeast Asian refugee populations. They conducted one study in a Thai refugee camp. Over 50% of Cambodian refugees (n = 993) met diagnostic criteria for depression, and an additional 25% met criteria for PTSD. Most refugees reported experiencing multiple acts of violence, loss, and deprivation (Mollica et al., 1993). McSharry and Kinney (1992) documented a 43% prevalence of PTSD among Cambodian refugees (n = 124) after living in the US between 12 and 14 years. Mollica and colleagues (1993) measured trauma exposure and PTSD symptomatology among a sample of Vietnamese survivors of torture (n = 51). They found 90% met diagnostic criteria for PTSD and another 49% met criteria for depression (Mollica et al., 1993). Mollica and colleagues (1993) point to a link between intensity of torture experienced by the individual (as indicated by the number of traumatic events endorsed) and severity of PTSD symptomatology.
Many researchers have described a dose-response relationship between trauma exposure and PTSD (Friedman, Keane, & Resick, 2007) and several have documented the phenomenon among refugee populations. Thabet and Vostanis (2000), for example, examined traumatic events and PTSD among a sample of Palestinian children living in the Gaza Strip. They found a positive relationship between the number of traumatic events experienced by the children and severity of PTSD symptomology. Forty-one percent of the sample met criteria for PTSD. Smith and colleagues (2008) conducted a large study on the mental health of Bosnian children (n = 3000) living in southern Bosnia-Herzegovina. They found an estimated PTSD prevalence of 52% and reported the degree of exposure to war related violence was the strongest predictor of PTSD.
El Sarraj, Pumamäki, Salmi, and Summerfield (1996) documented a 20% prevalence of PTSD among torture survivors living in Gaza. Shrestha and colleagues (1998) documented significantly higher rates of PTSD, anxiety, and depression among Bhutanese refugees (n = 526) compared to matched controls both living in Nepal. Researchers documented high rates of PTSD among: Central American adult refugees (Michultka, Blanchard, & Kalous, 1998), Sierra Leonean refugees living in the Gambia (Fox & Tang, 2000), and Sudanese refugee women (Kim, Torbay, & Lawry, 2007) and children (Paardekooper, de Jong, & Hermanns, 1999).
Pre-migration and post-migration stressors
Porter and Haslam (2005) conducted a meta-analysis of pre-migration and post-migration stressors associated with mental health outcomes of refugees. They documented significant pre-migration predictors of mental health outcomes including: age at the time of displacement (younger refugees seem to fare better than older refugees); gender (male refugees seem to fare better than female refugees); region of displacement (refugees displaced from urban areas seem to fare better than refugees displaced from rural areas); educational level (refugees with lower levels of formal education seem to fare better than refugees with higher levels of education); and socioeconomic status (refugees with lower pre-migration socioeconomic status seem to fare better than refugees with higher pre-migration socioeconomic status).
They also documented significant post-migration predictors of mental health outcomes including: living accommodations (refugees with permanent, private accommodations seem to fare better than refugees with institutional or temporary, private housing); economic opportunity (refugees with access to employment and ability to maintain pre-migration socioeconomic status seem to fare better than refugees with limited access to employment and marked loss of socioeconomic status); locus of displacement (externally displaced refugees seem to fare better than internally displaced refugees); repatriation status (permanently resettled refugees seem to fare better than repatriated refugees); and the stage of the conflict (refugees from conflicts that have since been resolved seem to fare better than refugees from conflicts that are ongoing). Refugees also report a multitude of migration stressors including loss of loved ones, shortage of food and basic necessities, exposure to war-related violence, and torture (Porter & Haslam, 2005).
Somali mental health
Like other refugee populations, Somali refugees experience high rates of exposure to adversity and are at risk for developing mental health disorders. Research has revealed generally high rates of depression, anxiety, and PTSD among Somali refugees. Roodenrijs, Scherpenzeel, and de Jong (1998) conducted one of the first studies on mental health disorders among Somali refugees. They measured symptoms of depression, anxiety, and posttraumatic stress in relation to the number of traumatic events experienced among Somali refugees (n = 54) resettled in the Netherlands and found that the most prevalent disorders were depression (63%), anxiety disorder (36%) and PTSD (31.5%). Depression and PTSD were comorbid in 7.5% of the sample. Pre-migration trauma strongly related to post-migration depression, anxiety, and PTSD, but no significant correlations were found between the number of traumatic events experienced and subsequent psychopathology.
Similarly, Bhui and colleagues (2003) studied traumatic events, migration characteristics, and psychiatric symptoms among 180 Somali refugees living in the U.K. About 22% of women and 28% of men met diagnostic criteria for comorbid anxiety and depressive disorders. Cumulative pre-migration trauma was a risk factor for both anxiety and depression. Traumatic experiences commonly associated with psychological distress included food shortage and being in a war-like situation. They found torture to be a non-significant contributor to psychopathology. In fact, individuals who were exposed to combat or imprisonment actually exhibited a lower risk for depression, anxiety, and suicide in this study. Bhui and colleagues suggested the findings might reflect resilience factors not yet represented in the literature (Bhui et al., 2003).
Jaranson and colleagues (2004) conducted an epidemiological study of torture prevalence and related problems among a community-based sample of Somali and Oromo refugees (n = 622) living in the Midwest US. They found a 36% prevalence of torture among the sample, a higher rate of torture than typically reported in the literature. Women reported torture experience as often as men and all but six participants reported traumatic experiences. Both trauma and torture positively associated with social, physical, and psychological problems. Social problems were more common among women and individuals who reported decreased religious practice. Social problems were less common among individuals with English language fluency, who had a high school diploma/GED, who had lived in the US longer, who were employed, and those who were homeowners.
Halcón and colleagues (2004) investigated life circumstances, health, and trauma history among a sample of Somali and Oromo youth (n =338) living in the US. Overall, they found higher rates of trauma exposure strongly associated with psychological and physical difficulties but only weakly associated with an increase in social problems. Men reported more physical and PTSD complaints than women, whereas women endorsed more social problems. Robertson and colleagues (2006) found that symptoms of PTSD among Somali and Oromo women (n = 459) significantly correlated with older age, a larger family, an absent spouse, and caring for children while living alone.
Bhui and colleagues (2006) examined anxiety, depression, and PTSD among a sample of Somali refugees (n = 143) in the early stages of resettlement in the U.K. They were interested in rates and correlates of comorbid anxiety and depression and PTSD. About 35% of the sample met criteria for anxiety or depression (referred to by the authors as common mental disorders) and 14% met criteria for PTSD. The researchers noted higher risk of mental disorders among asylees, users of khat (a flowering plant native to the horn of Africa that is chewed for stimulant-like effects), and recruits from primary care settings. They found lower risk of mental disorder among individuals who were educated and employed. Overall, 30% of participants met criteria for a depressive disorder and 80% of participants who met diagnostic criteria for PTSD also met criteria for anxiety or depression. These findings suggest that the comorbidity of depression, anxiety, and PTSD is so high that it is difficult to measure them as discrete disorders among Somali refugee populations.
Cross-cultural comparison studies
Cross-cultural research comparing rates of psychopathology among Somali refugees to other refugee populations is slight, but interesting. Strutters and Ligon (2001), for example, found anxiety to be highest among Somali refugees when compared to refugees from either Yugoslavia or Vietnam. Gerritsen and colleagues (2006) compared rates of depression, anxiety, and PTSD between three groups of refugees and asylum seekers from Afghanistan, Iran, and Somalia and found that while Somali refugees and asylum seekers experienced the greatest number of traumatic events (M = 7.6, SD = 3.9), they also reported the lowest levels of depression, anxiety, and PTSD. Among all refugee groups, however, an increase in the number of traumatic events experienced was associated with an increase in psychological distress; greater post-migration stress; and low social support was also related to increased anxiety, depression, and posttraumatic symptomology (Gerritsen et al., 2006).
Kroll, Yusuf, and Fujiwara (2011) examined PTSD, psychosis, and depression among an outpatient clinical sample of 600 Somali refugees living in the US. They compared prevalence of these disorders to a cohort sample of 3,009 non-Somali patients after observing a seemingly high rate of Somali refugees reporting psychotic symptomology. Overall, Somali refugees experienced significantly higher rates of depression and psychosis compared to non-Somali patients, while rates of PTSD did not differ significantly between the two groups. Interestingly, 80% of Somali men under age 30 in the sample were diagnosed with a psychotic disorder. These rates decreased with age; about 40% of Somali men ages 31-50 were diagnosed with a psychotic disorder and only 8% of men over age 50 were diagnosed with a psychotic disorder. Somali women were diagnosed with psychosis at a much lower rate (32%). This rate, however, was still significantly higher in Somali women compared to non-Somali women (14%) in the sample. In the same study, only 3% of Somali men under the age of 30 met diagnostic criteria for PTSD. This number increased with age resulting in 15% prevalence among men over 50 years old. Likewise, only 9% of women in the study met criteria for PTSD, with the prevalence rate remaining relatively stable across age groups.
The authors explained the low rates of PTSD were likely due to young Somali men’s reluctance to acknowledge or discuss past traumas. When trauma was acknowledged, the authors described a strong denial of emotional impact or lasting effects of witnessing or experiencing the traumatic event. Men and women alike denied sexual violence against women despite contrary evidence elsewhere in the literature (Jaranson et al., 2004).
Post-migration adaptation
Post-migration adaptation is a key factor in psychological well-being after resettlement (Ingleby, 2005). Political, social, physical, and psychological factors may prevent refugees from adapting to life in their host country. The process of relocation puts refugees at risk for problems due to stress, acculturation problems, employment status, individual personality characteristics, and traumatic experiences during the various stages of migration (Bhugra, 2004; Williams & Berry, 1991). Several studies have pointed to post-migration mobility in the host country as a significant factor associated with mental-health status of Somali refugees (Palmer, 2006; Warfa et al., 2006). For example, changes in residential status within the first five years for Somali refugees living in the U.K. was strongly related to depression after controlling for area of residence, age, and gender (Warfa et al., 2006). Moreover, Silveira and Allebeck (2001) linked loss of social status (e.g., vocational status) to increased depression in older Somali male refugees.
Young (2006) examined the role of acculturation in psychological adjustment among a sample of Somali refugee women living in Canada. She found a longer residence in Canada related with increased perception of discrimination, both individually and collectively as a Somali. Finally, Halcón and colleagues (2004) studied the current living situations of 140 Somali refugees living in the US and found that 21% of males and 6% of females reported living alone, 51% of men and 38.5% of women participants reported problems getting a job, and half of men and nearly half of women reported difficulty adjusting to life in the US. Nearly half of all women and one-third of all men in the sample reported feeling alone since migration. The majority of Somali participants, however, reported receiving more respect in the US than in Somalia, and about 80% reported having made the correct choice in migrating to the country.
Although protective factors have not been the focus of any quantitative study of Somali refugees, several studies have alluded to potential protective factors that may buffer the impact of risk factors on the development of mental health disorders. Bhui and colleagues (2006), for example, found that greater educational experience and employment in the host country related to lower risk for anxiety, depression, and PTSD. Halcón and colleagues (2004) reported that fluency in English, immigration at a younger age, immigrating to the US with a family member, and a longer time living in the US all significantly related to lower PTSD scores among Somali refugees. Moreover, Silveira and Allebeck (2001) identified support from their family, interaction with peers, and engagement in religious practices as protective factors against depression for Somalis.
In sum, the UNHCR documented 43.7 million forcibly displaced persons living worldwide at the close of 2010 (UNHCR, 2010). Refugees experience high rates of mental disorders and social problems due to a constellation of pre-migration and post-migration stressors and psychological tendencies. Many factors seem to contribute to poor mental health outcomes, including age, gender, region of displacement, educational level, socioeconomic status, living accommodations, economic opportunity, locus of displacement, repatriation status, and stage of the conflict. Post-migration adaptation is a key factor in psychological well-being after resettlement (Ingleby, 2005). Political, social, physical, and psychological factors may promote or hinder adapting to life post-migration. Although protective factors have not been the focus of any quantitative study of Somali refugees, several studies have alluded to potential protective factors that may buffer the impact of risk factors on the development of psychopathology.
Resilience is a term used to capture the processes, predictors, and outcomes related to positive adaptation in the context of adversity. Instead of focusing on problems and disorders, resilience focuses on solutions and health promotion. The following section presents a brief history of resilience research, cultural and contextual considerations for the study of resilience, and an overview of the IRP.
Resilience
The term resilience comes from the Latin word resile, which means “to leap back.” Early conceptualizations of resilience typically emphasized individual or individually mediated factors associated with positive outcomes in the context of adversity (e.g., Anthony & Cohler, 1987). Anthony and Cohler’s (1987) work on ego-resilience marks the early research on the construct. Ego-resilience is a multidimensional personality trait largely dependent on intellect and behavioral temperament (e.g., a sunny disposition) and expressed through one’s ability to see multiple perspectives, plan for the future, express creativity, and maintain a sense of humor—even in the context of adversity (Anthony & Cohler, 1987).
Confusion between the term ego-resilience and resilience more broadly defined has contributed to criticism of the construct as a tautology. Indeed, ego-resilience is closely related to the personality construct hardiness (Kobasa, 1979), and measurement in this context offers little additional information outside of this well-established psychological construct (Waaktaar & Torgersen, 2010). Much of the research on ego-resilience, therefore, falls outside of the parameters of contemporary conceptualizations of resilience, as the narrow conceptualization largely overlooks the potential influence of environmental factors. Longitudinal research, however, has elucidated the role of environmental factors on development of psychopathology in addition to individual-level factors.
Brief history of resilience research
Garmenzy and colleagues’ (1984) longitudinal study investigated developmental risk factors for psychopathology and the effects of stressful life events on the functional competence of children considered at-risk for psychopathology. The study captured an outlier group of at-risk children who experienced marked deficiencies in functional competence (as measured by social competence and attentional functioning). Surprisingly, the majority of at-risk children in the study displayed adaptive social behavioral patterns and work achievement and presented little to no indication of psychopathology or social incompetence over time (see Garmenzy & Devine, 1984; Nuechterlein, Phipps-Yonas, Driscoll, & Garmezy, 1990 for details). Positive engagements in the classroom and academic achievement were both associated with positive adaptation (i.e., adaptive social behavioral patterns and work achievement) among the at-risk sample; however, the relationship between both of these variables and positive adaptation was moderated by overall intelligence. Moreover, socioeconomic status and social support (family and community) were also related to positive adaptation.
The Kauai study was another longitudinal investigation of resilience, which examined human development from birth to midlife among a cohort of 698 infants born on the Hawaiian island of Kauai in 1955 (Werner & Smith, 1982; 2001). According to Werner and Smith (1977), over one-third of the Kauai study sample experienced marked risk factors or adversity during childhood. Of this at-risk sample, two-thirds developed a learning disability, mental health problem, or behavioral problems by age 18. The remaining one-third developed into competent, well-adapted adults. As children and adolescents, none of these participants developed a learning or behavioral disorder; they all did well in school, managed home and social life adequately, and set realistic educational and job goals. By age 40, all of these individuals were employed, none had a history of legal trouble, and all were financially self-sufficient. Divorce rates were low in this subpopulation of at-risk participants, mortality rates and rates of health problems were significantly lower than their same sex peers, and their educational and vocational accomplishments equaled (even surpassed) those of children who grew up in economically secure and stable home environments (Werner & Smith, 2001).
The Kauai study elucidated the pervasive effects of early childhood relationships on subsequent developmental outcomes, as well as the role of internal locus of control and communication skills in moderating the relationship between risk and poor developmental outcomes (i.e., poor academic achievement). The study continues to explore the impact of biological and psychosocial risk factors, stressful events, and protective factors on human development (Werner & Smith, 2001), with the most recent report from the study highlighting the interactional effect of perinatal stress on the quality of family environment as well as the antecedents and consequences of childhood mental health problems and disabilities. This report links social class and vulnerability, and likelihood of persistence of childhood disorders, with biological and temperamental underpinnings (Werner & Smith, 2001).
Researchers have learned a great deal in the past several decades about protective factors that seem to buffer the impact of severe adversity. The Search Institute has developed lists of developmental assets specific to particular age groups that are associated with positive development. These lists have been integrated into educational programming and parent education programs across the US (Scales & Roehlkepartain, 2003). Each list includes external assets (e.g., support, empowerment, boundaries and expectations, constructive use of time) and internal assets (e.g., commitment to learning, positive values, social competencies, and positive identity), which differ slightly according to age. The developmental assets lists are available in 14 different languages on the Search Institute website (http://www.search-institute.org/developmental-assets/lists). The developmental assets movement calls attention to factors that are associated with positive development among all people, and these assets can be utilized to promote well-being and prevent problems (Scales & Roehlkepartain, 2003).
The notion of resilience evolved largely in a Western context with little consideration for cultural or contextual dimensions of the construct (Liebenberg & Ungar, 2009). Positive adaptation is typically operationalized based on Western assumptions and norms. Protective factors identified in the literature are based on research primarily conducted in Western contexts. A few notable exceptions involve qualitative investigations of resilience factors in several non-Western contexts and point to the need to understand adaptation as influenced by culture and context (Apfel & Simon, 2000; Felsmen, 1989; Klevens & Roca, 1999; Rousseau, Said, Gangé, & Bibeau1998a; Whittaker, Hardy, Lewis, & Buchan, 2005).
International Resilience Project (IRP)
Researchers at RRC conducted the IRP to begin to address the lack of research on resilience among non-Western populations. As previously mentioned, the IRP was a multisite, cross-cultural investigation of resilience among youths living in developing nations or among marginalized populations within developed nations (Ungar & Liebenberg, 2009). The IRP developed and pilot tested the Child and Youth Resilience Measure (CYRM), which was later adapted into the RRC-ARM. The IRP concluded the CYRM was a valid measure of resilience, appropriate for use across cultures and contexts.
The IRP concluded neither qualitative nor quantitative methods alone can completely capture resilience. Culture is captured well through qualitative methodology. One can observe and document the tone and tempo of narrative, the environment in which the interview took place, behavioral and interpersonal characteristics that shaped the interview experience. These factors can be easily lost in quantitative data, and often these factors are even controlled for methodologically. Qualitative data can provide honesty to research conclusions and contextualize our understanding of quantitative data. The IRP produced a contextual definition of resilience:
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways (Ungar, 2008, p. 225).
This definition includes the process of navigating and negotiating for health-sustaining resources. This inclusion highlights the dynamic nature of resilience and distinguishes it from more static explanations, such as those defined by outcome variables (e.g., school success) or culturally independent processes. The term navigation relates to individual capacity (or personal agency) to seek health-sustaining resources, as well as availability of those health-sustaining resources. One can only navigate toward experiences that are available and accessible to them (Ungar, 2008). The term negotiation refers to provision of health-sustaining resources in ways that are meaningful to the individual. In other words, individuals negotiate for resources that members of their culture consider health-enhancing. Resilience as a process can be examined through qualitative data. Processes explain how more static factors work together to promote culturally meaningful pathways toward the experience of health and well-being in the context of adversity (i.e., resilience).
Health and well-being, of course, are also culturally embedded experiences, and resources are contextually bound. Careful consideration should inform selection of outcome markers when conducting cross-cultural investigations. A common outcome marker of resilience across studies among youth, for example, is staying in school. Indeed, staying in school is reflective of positive adaptation in a typical Western context and is likely an appropriate outcome variable with shared meaning within this context. In some non-Western contexts, however, staying in school may not be as important. Working the family farm in order to earn enough income to meet basic needs of the family may be more important than staying in school. Measuring educational attainment in this hypothetical context may lack cultural relevance as a marker of resilience. Identifying culturally valued and contextually relevant markers of resilience is essential to culturally-relevant investigations of resilience.
Four propositions for the study of resilience
The IRP offered four propositions useful to the contextualized study of resilience (Ungar, 2008). Each proposition builds on the other, concluding in the presentation of seven tensions through which resolution (using four common strategies) results in the experience of resilience.
Proposition One states resilience has universally and culturally and/or contextually specific dimensions. Ungar (2008) explains how individuals share a common set of characteristics and processes related to resilience. The IRP produced reliable and valid quantitative data across cultures; but, they were unable to produce a universally valid factor structure.
Proposition Two states various dimensions of resilience exert differing amounts of influence on an individual’s life depending on the culture and context in which resilience is realized. Ungar (2008) explains how understanding the amount of influence a particular aspect of resilience exerts on well-being is difficult to determine, particularly through quantitative methods alone.
For example, comparing mean scores (on a 5-point scale) on the CYRM item ‘Are religious or spiritual beliefs a source of strength for you’ across three different contexts, Sheshatshiu (M = 1.7), Halifax (M = 2.64), and Palestine (M = 4.44), may lead to the conclusion that religious beliefs are of greater importance to Palestinian youth compared to youth in the other two contexts. What is unclear based on quantitative data alone, however, is whether higher endorsement of the item by Palestinian youth represents a greater influence on resilience given Palestinian culture and context, or whether higher endorsement simply reflects cultural relevance, not necessarily influence. Palestinian youth may simply be surrounded in more religious and spiritual expressions of culture leading to greater endorsement of the item. Measuring any aspect of resilience in one context may or may not relate to measurement of the same aspect of resilience in another context (Ungar, 2008).
Proposition Three states that aspects of individuals’ lives that contribute to resilience are related to one another in patterns that reflect individuals’ culture and context (Ungar, 2008). Rather than neatly sorting into individual, relational, communal, and cultural aspects of healthy functioning, aspects of resilience link together thematically in different ways depending on the culture and context in which individuals reside. For example, Ungar and colleagues (2007) hypothesized CYRM items related to self-efficacy would load at the individual level. They found that response patterns on the CYRM linked individual-level self-efficacy, with self-efficacy in relationships, in the community, and in the cultural context (e.g., political efficacy).
Proposition Four states that individuals who successfully resolve the seven tensions (viz., access to material resources, relationships, identity, power and control, cultural adherence, social justice, and cohesion) are those who experience themselves, and are seen by their communities, as resilient. These seven tensions emerged from IRP qualitative data analysis. There is not a prescriptive way in which individuals successfully navigate through these tensions. It is the fit between the attempted solutions and how well the solution resolves the challenges posed by each tension, within the norms of each community (Ungar, 2008). See Table 1 for a summary of the seven tensions described by the IRP.
Table 1
Seven Tensions
| Tension | Explanation |
| Access to Material Resources | Availability of financial, educational, medical and employment Assistance and/or opportunities, as well as access to food, clothing and shelter |
| Relationships | Relationships with significant others, peers and adults within one’s family and community |
| Identity | Personal collective sense of purpose, self-appraisal of strengths and weaknesses, aspirations, beliefs and values, spiritual and religious identification |
| Power and control | Experiences of caring for one’s self and others, the ability to effect change in one’s social and physical environment in order to access health resources |
| Cultural adherence | Adherence to one’s local and/or global cultural practices, values, and beliefs |
| Social justice | Experiences related to finding a meaningful role in community and social equality |
| Cohesion | Balancing one’s personal interests with a sense of responsibility to the greater good; feeling a part of something larger than ones’ self socially and spiritually |
Note. Reprinted from Ungar, 2008, p. 231
Ungar (2008) identified four principles that govern the resolution of the seven tensions. First, individuals can only select from available and accessible health resources. Second, individuals will choose the available health resources that are most likely to influence their health positively (as determined by culture and context). Third, the way individuals relate one aspect of resilience to another will reflect similarities and differences in how individuals behave across cultures. And fourth, relationships between aspects of resilience will be expressed differently within and between populations.
To provide a context through which to consider cultural implications of the present study, an overview of Somali culture is presented next.
Somali Cultural Profile
Somalia is a country located in the northeastern corner of the African continent in a region commonly referred to as the horn of Africa. The country is roughly the size of Texas and has the longest coastline on the African continent. The Indian Ocean is to the east and the Gulf of Aden to the North; the country of Djibouti borders to the north, and Ethiopia and Kenya border to the west and southwest respectively (Putnam & Noor, 1993). The climate of Somalia is very hot and dry, although the higher elevations in the northern part of the country offer cooler temperatures (Putnam & Noor, 1993). This semi-arid to arid environment is conducive to nomadic pastoralism, a form of agriculture practiced by over 50% of the Somali population, in which livestock are herded either continuously or seasonally in search of fresh pastures for grazing. Somali people are also fishermen and seafarers, farmers, and urban businesspeople (Putnam & Noor, 1993).
Culturally, Somali people may be a group for whom Western conceptualizations of mental health treatment are not intuitive (or applicable). According to Schuchman and McDonald (2004), Somali people are traditionally unfamiliar with the concept of mood disorders, such as dysthymia or depression. Mental illness is viewed as a dichotomous construct – either the person is crazy (waali) or not. Somali conceptualizations of mental illness can involve spiritual or metaphysical explanations, and Islam seems to provide an explanatory model for human suffering at the individual and collective level (Koshen, 2007).
Religion
Nearly all Somali people practice Islam, and the religion serves as a unifying force across the country. According Koshen (2007), Islamic teachings suggest all events are of God’s will and are therefore out of individual control. Therefore, some Somali people conceptualized the suffering and social turmoil as God’s punishment for straying from the Islamic path. The way to get back on path is to collectively redirect the society toward Islamic law (Koshen, 2007). The increase in more fundamentalist interpretations of Islam may partially be the result of this conceptualization. Islamic fundamentalists advocate for Shari’ah law (law based on the Quran), which is passed down orally through generations and is thought to preserve basic values in Somali society (Koshen, 2007). Shari’ah law traditionally guided management of communal land and pastures, conflict management and prevention, family law and justice, and diya (the paying of blood money; see Putnam & Noor, 1993 for more details).
Language
A rich oral tradition is an essential component of Somali culture. According to Mire (2007), knowledge of all forms of social life and expression were traditionally transmitted from generation to generation through oral tradition. Poets were the keepers of the clan history, including their relations with other tribes. Poets often acted as a form of mass media, sharing information and public opinion (Mire, 2007). The Somali script was written in 1972 and the Barre administration launched a massive literacy campaign across rural and urban Somalia, purporting to raise the literacy rate to 55% (from 5% prior to the campaign; Putnam & Noor, 1993). Interestingly, Koshen (2007) observed how younger generations of Somali people are more likely to be literate in Somali and English, whereas older generations of Somali people are likely to be illiterate in both Somali and English. Moreover, people born after 1972 are less likely than their older counterparts to speak any other language (e.g., Arabic, Italian, Swahili; Putnam & Noor, 1993).
Social structure
Somali people belong to a patrilineal society, and their clans and subclans identify everyone (Abdullahi, 2001). This fact is reflected in the common Somali question, tol maa tahay, which means, what is your lineage? The clan identity forms the foundation of social structure in Somalia – clan identity defines relationships, rights, and obligations (Koshen, 2007). Illustratively, children are taught to memorize and recite their genealogy backwards along the male bloodline (fathers, grandfather, etc.) until they reach the founding father of the clan, which is often up to twenty generations back (Koshen, 2007).
According to Putnam and Noor (1993), there are two overarching clans in Somalia: Samaale and Sab. Samaale are the majority group and consist of four main subclans: Dir, Isaaq, Hawiye, and Daarood. Each of these subclans is divided into additional subclans. Samaale are primarily of nomadic ancestry and live across east Africa. Sab have two main subclans: Digil and Raxanweyn. Sab live mainly in southern Somalia and mix farming and herding, making them more likely to live a sedentary lifestyle than Samaale (Putnam & Noor, 1993). Clan stability is unpredictable, and changing alliances and temporary coalitions are common.
Family
Five Islamic prescriptions define Somali family structure. First, marriage is a religious duty and social necessity. Second, sex outside of marriage is prohibited. Third, the husband is obligated to provide for his wife. Fourth, the wife must obey her husband. And fifth, family members are obliged to be kind to relatives and express concern for their well-being (Houseknecht & Pankhurst, 2000, as cited in Koshen, 2007).
Somalis tend to value family, and the family serves as a source of support and security during difficult times (Koshen, 2007). It is not unusual for a Somali family to have seven or eight children, and household composition typically involves extended family members and often exceeds ten persons. Extended family includes paternal and maternal relatives and people who are several times removed and belong to another clan (Koshen, 2007). Nurturing Islamic values in children is of primary importance, and children are granted incremental duties in the family along gender lines (Abdullahi, 2001).
Gender roles
Somalia is primarily a male-centered society in that men are responsible for clan and family decision-making, at least publically. Women do, however, play an essential economic role in farming, herding, and business in the city, and men often seek counsel from women regarding important decisions (Putnam & Noor, 1993). Division of labor in pastoral life is clearly defined. Men are responsible for the safety and security of their herd, and they travel long distances scouting for water and fresh pastures on which the herd can graze. Women are responsible for domestic work, caring for the children and elders, loading and unloading camels, raising and taking apart the traditional shelter (awal), and keeping count of the livestock (Koshen, 2007).
Marriage in Somalia was traditionally arranged. Marriages across clans were encouraged as these strengthened alliances across clan groups; however, one of the consequences of the Civil War is that women are more likely to marry within the clan or sub-clan to reduce their chances of falling victim to inter-clan conflicts (Koshen, 2007). After marriage, women maintain their legal rights with their agnatic group (i.e., their father’s clan group). These rights serve to protect her well-being. If a husband were to mistreat his wife and the woman was in distress, for example, her kinsmen are responsible for providing her material assistance, and they may seek compensation from the husband’s clan. Likewise, if the wife were to commit a crime, her kinsmen would be responsible for paying compensation (Koshen, 2007).
Health and health-sustaining resources
According to the United Nations Human Development Report (UNDPR, 2001), the average life expectancy in Somalia was estimated at 47 years old, with women living slightly longer than men. The infant mortality rate and the under-five mortality rate are among the highest in the world (132 and 224/1,000 live births, respectively). At the time of the report, only 28% of people living in Somalia had access to any form of modern health services, and there were only 0.4 doctors per 100,000 persons living in the country (UNDPR, 2001). Little is known about the health and well-being of people living in Somalia.
History of Somali Civil War
The Somali Civil War started roughly in 1991 with the collapse of the Said Barre regime (Abdullahi, 2001). A drought settled over East Africa at about the same time, and food and power fell into the arms of those with guns. Over the course of one year, hundreds of thousands of Somali people died from violence, disease, and famine (Putnam & Noor, 1993). In 2011, the UNHCR reported alarming deterioration with regard to the situation in Somalia yet again. The number of Somali refugees arriving in neighboring Kenya, Ethiopia, and Yemen during the first quarter of 2011 was reportedly double that of the number during the first quarter of 2010 (50,000 from 25,000, respectively). Another drought settled over East Africa in 2011 (said to be the “deadliest in 60 years”), leading to widespread famine and fueling the ongoing political violence. News emerged recently (September, 2012) from Somalia of an elected government now formally recognized by the United Nations. This is the first formally recognized government in Somalia in over 20 years.
Study Aims
Now that an overview of Somali history, culture, and current sociopolitical context has been presented, I will next present a brief discussion of studies on resilience among Somali refugees, leading to a presentation of this dissertation’s study aims. As mentioned previously, only two studies have explicitly examined resilience with Somali refugees, and both were qualitative studies. Rousseau and colleagues (1998a) conducted an ethnographic exploration of resilience with a historically high-risk group of refugees – unaccompanied minors. They analyzed the collective mechanisms of the pastoral society of Northern Somalia that “put the resistance and ability of young refugees to the test” (Rousseau et al., 1998a, p. 161). Using ethnographic data and storytelling, the authors showed how the collective meanings attributed to early separation from family (e.g., learning, positive development) served as a protective factor, buffering the impact of later separation from family due to the Civil War and violence.
In the context of pastoral life in Northern Somalia, children are first assigned their own role in pastoral life around the age of five. The child begins to look after the small animals in and around the camp. Gradually assuming more responsibility, the young men become apprentice camel drivers (dabadonn) at the age of 12. This involves participation in the practice of transhumance (hergeeline) and the experience of lengthy separations from their community and family. During hergeeline, the dabadonn (like his seniors, the geeljirs) must abstain from eating or drinking all day long and wait until all of the camels are milked before feeding himself in the evening. The memories of exhaustion, hunger, and perseverance are firmly implanted in a young man’s early experience. The dabadonn lives with his peer group during the months of separations, as they ensure survival during these months through emotional support and shared experience.
Separation from family in pastoral life is associated with learning and positive development. A boy cannot become a man until he is able to endure the hardship of hergeeline, and gains full acceptance as a man only after he marries. Rousseau and colleagues (1998a) suggest the meaning linked with culturally mandated separation may serve as a protective factor, essentially buffering Somali men from the negative effects of stress later in life. Rousseau and colleagues’ (1998a) qualitative finding offers a contextually bound explanation related to subsequent expressions of resilience (e.g., positive adaptation in the context of forced displacement).
In the second study of resilience among Somali refugees, Whittaker and colleagues (2005) examined the psychological well-being of Somali refugee women living in Northern England. They defined psychological well-being in terms of positive emotional and mental health, life satisfaction, positive affect (happiness), and coping abilities, and they considered the construct (well-being) through social, political, and psychological lenses.
The participants described the importance of moving on, being strong, not dwelling on the past, and coping as essential components of psychological well-being, and they sought support from family, friends, and professional services. However, the women also discussed the need for concealment of mental health problems from others in their community due to stigma associated with mental illness. Refugee populations often report resistance toward engaging in research focused on psychopathology due to culturally embedded stigma related to mental illness (Ingleby, 2005). Whittaker and colleagues (2005) demonstrated how this stigma might play a role in the Somali refugee community as well.
The present study extends the literature on Somali conceptualization of resilience and the work of the IRP by administering the RRC-ARM to a sample of Somali refugees living in the US and exploring dimensions of resilience in the context of Somali culture and forced displacement. A participatory, sequential, mixed-method design was chosen for this study in order to capture both depth and breadth of information about resilience in this context. The research design included three broad phases. During phase one, we conducted interviews with resilient Somali people (n =10) living in the US about experiences of health and well-being in the context of adversity across three distinct contexts (i.e., Somalia, refugee camps, US).
We sought to answer the following research questions during phase one to gain contextual information about resilience in the context of Somali culture and forced displacement:
- How do “resilient” Somali refugees currently living in the US conceptualize resilience?
- What resources contribute to resilience processes and outcomes, health and well-being?
- How does context and culture shape the experience of health and well-being?
These interviews produced rich descriptions of resilience and well-being and formed the backbone for a quantitative investigation (phase three) of resilience. During phase two, we selected study measures for phase three based on findings from phase one. Also, during phase two, we engaged in an iterative process of translation, back-translation, and cultural adaptation of all study measures. During phase three, we administered a quantitative survey of life difficulties (PMLD), well-being (PWI-A), meaning in life (MLQ), and resilience (RRC-ARM) to a sample of Somali refugees (n = 137) living in the US. We sought to answer the following research questions in phase three:
- What kind of factor structure can be established for a measure of resilience among Somali refugees?
- Can enough evidence be produced to support the reliability of the RRC-ARM?
- Can enough evidence be produced to support the construct validity of the RRC-ARM?
- Can enough evidence be produced to support the incremental validity of the RRC-ARM?
Qualitative and quantitative data were analyzed separately and then integrated into a proposed Somali Multilevel and Multidimensional Resilience (SMMR) model.
Chapter 3: Research Design and Methodology
Overarching Study Design
This study employed a participatory, sequential, mixed-method research design to examine resilience in context of Somali culture and forced displacement. Cultural advisors participated during each phase of the study. Mixed-methodology (qualitative and quantitative) allowed for examination of resilience with both depth and breadth (Onwuegbuzi & Leech, 2005). The study involved three broad phases, depicted by Figure 2.
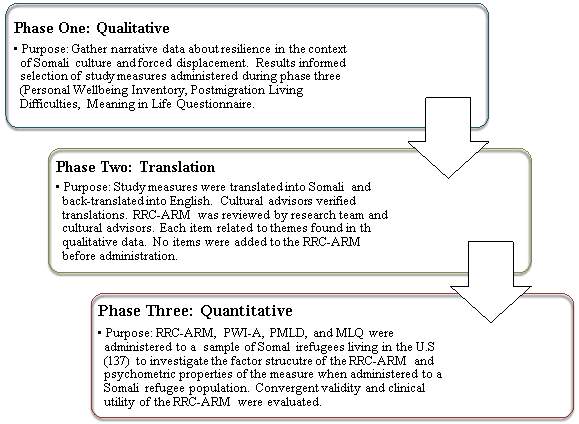
Figure 2. Three-phase research design
Cultural Advisors
As recommended by Ungar and Liebenberg (2009), three cultural advisors oversaw all phases of the project. Most importantly, cultural advisors contributed to the selection of study variables considered culturally relevant and respectful of participant and cultural boundaries. Cultural advisors’ feedback was taken seriously and resulted in several key changes to research design. For example, when this study was originally conceptualized, the key variables of interest were resilience, depression, and anxiety disorders. However, the cultural advisors suggested that measurement of mental disorder might serve as a disincentive to participation in the study. They recommended selection of a positive psychological construct, such as well-being. Thus, the Personal Well-being Index-Adult (PWI-A) was selected as a substitute for measurement of disorder.
Cultural advisors participated in a variety of other ways, including:
- Co-conceptualizing the research project;
- Reviewing key-informant interview protocol and making recommendations for revisions;
- Consultation on key-informant interviews and codebook development;
- Translating and verifying study measures and adapting the study measures, consulting on the survey format;
- Facilitating connections with community organizations who helped facilitate quantitative data collection;
- Interpretation and presentation of research findings.
Meetings with advisors occurred as needed, most typically in the form of telephone conversations, followed by email communications. Somali cultural advisors consisted of one male living in Anchorage, Alaska, and one man and one woman living in Minneapolis, Minnesota. These advisors were chosen because of their own experience overcoming adversity and their understanding of Somali culture, language, and community. Many other Somali community members, as well as many academic and professional consultants, were less formally involved in shaping the project.
Human Subjects Protection
In compliance with Federal Laws and Regulations (42 CFR, Part 2), all aspects of the qualitative and quantitative data collection and analysis adhered to strict confidentiality policies and procedures. The University of Alaska Anchorage Institutional Review Board (IRB) reviewed all procedures and measures used in this study to ensure the highest ethical standards were respected. All participants were informed of the purpose of the study, what was expected of them if they chose to participate, efforts to ensure confidentiality, and were provided an opportunity to withdraw from the study. If a participant chose to be in the study, he/she was asked to sign informed consent (electronically or in-person depending on the phase of the project as described below) and was reminded that he/she could withdraw from the study at any point without penalty. This study followed all guidelines for the protection of data, including limited access to the data. Data were stored in a locked file room with locked fireproof file cabinets at the University of Alaska Anchorage, and de-identified data were stored in password-protected files on a secure password-protected computer, accessible only by the research team.
Phase One: Qualitative Data Collection and Analysis
A qualitative phase was implemented to gather information about resilience in the context of Somali culture and forced displacement. In-person, key-informant interviews with resilient Somali people (i.e., those who have adapted well per the conceptualization of the individual identifying the participant despite exposure to significant adversity) living in Minnesota and Alaska were conducted. Phase one data collection and analysis addressed the following broad research question: How is resilience conceptualized in the context of Somali culture and the refugee experience? More specifically, phase one data collection and analysis sought to answer:
- How do “resilient” Somali refugees currently living in the US conceptualize resilience?
- What resources contribute to resilience, processes and outcomes, health and well-being?
- How does context and culture shape the experience of health and well-being?
Sampling and recruitment
Participants were selected using a snowball sampling technique. Snowball sampling is a non-probability sampling technique where study participants recruit future study participants from among their acquaintances (Denzin & Lincoln, 2008). Snowball sampling is often employed when populations are challenging to access, such as resilient Somali refugees living in the US. As participants are not selected from a sampling frame, snowball sampling is subject to a number of biases that may limit the generalizability of the findings of the study. In this study, however, the snowball sampling strategy was employed in such a way to maximize Somali perspectives on resilience, thus the “bias” may actually increase the trustworthiness of the data.
Qualitative data collection was limited to English-speaking participants. While this is an important limitation, the choice to include only English-speaking participants was based on limited resources for interpretation and the potential errors that may occur during interpretation and transcription of interpreted data. Table 2 depicts inclusion criteria for phase one of the study.
| Table 2
Inclusion Criteria for Phase One: Qualitative Data Collection |
|
| Criteria | Requirement |
| Age | 18 or older |
| National origin | Somalia |
| Ethnicity | Somali or Bantu |
| Present location | United States |
| Language | English |
The director of the Refugee Assistance and Immigration Services (RAIS) program in Anchorage, Alaska identified the first key-informant residing in Alaska, and the director of the Somali and East African Behavioral Health (SEABH) program in Minneapolis, Minnesota identified the first key-informant living in Minnesota based on a set of inclusion criteria (see Table 3) and the following definition of resilience: an individual who has adapted well (e.g., not seriously mentally ill, engaged in meaningful life activities) despite exposure to significant adversity. Each director assisted with scheduling the first interview by making phone contact with the potential key-informant, introducing the project, and facilitating an introduction to the research team, as well as by providing a priori information regarding culturally expected behavior during the interviews (e.g., with whom to shake hands). Interviews occurred at mutually agreed upon community locations, maximizing the opportunity to enter the participant’s community context.
Each participant was asked to identify another “resilient” Somali refugee (who met inclusion criteria for the study) per his/her personal definition of resilience discussed during the interview, and asked to facilitate communication and scheduling with the potential key information. The snowball sampling strategy aimed to capture a group of people identified as resilient from conception of their peer and cultural group. The snowball sampling strategy is pictorially presented in Figure 3.
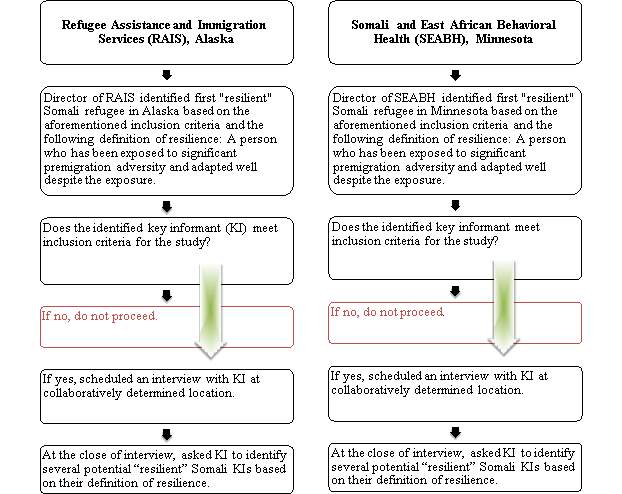
Figure 3. Snowball Sampling Strategy
Participants
Qualitative data were collected through individual semi-structured interviews with “resilient” Somali refugees living in Minnesota (n = 6) and Alaska (n = 4), ranging in age from 22-56 (M = 37.5, SD = 12.45) and equally distributed by gender. One hundred percent of the sample identified as Muslim and most reported being married (60%). All 10 key-informants were born in Somalia and migrated to the US within the last 30 years. Most key-informants reported spending time in refugee camps (70%) with an average length of stay in refugee camps of 4.35 years (SD = 5.77). Three men (ages 45, 45, and 41) and one woman (age 22) came to the US from Somalia or other African countries where they were studying abroad prior to the civil war. Seven of the 10 key-informants identified as citizens of the US.
Data collection procedure
Prior to the start of the interview, the interviewer provided the key-informant with an informed consent in English. The interviewer verbally informed the key-informant of the purpose of the study and of the voluntary and confidential nature of the study. The interviewer invited questions from the key-informant and made sure he/she understood the purpose of the interview. Once informed, key-informants were asked to provide written consent. With permission from the key-informant, the interview was audio-recorded and transcribed verbatim for analysis.
Following informed consent, the key informant was asked to complete a demographic questionnaire (i.e., age, gender, marital status, religious orientation, level of education, nationality, refugee status, number of years in the US, length of stay in refugee camps, location of camp). Following collection of demographic information, the interview began. The interviews were semi-structured and lasted between 30 minutes to 2 hours. Once the interview was over, the key informant was thanked and given $20 as a token of appreciation for her or his time. See Appendix B to review the key informant interview checklist.
Interview protocol
The interview protocol was semi-structured allowing for exploration of unexpected issues while maintaining a core set of questions to guide the interview. The protocol included 10 questions designed to capture explanatory models of resilience according to Somali culture and context (e.g., “Describe a Somali person who lives well despite the many difficulties they face” and “How do you keep healthy?”), and roughly followed the recommended questions provided by Ungar and Liebenberg (2009).
The interview protocol was revised over the course of data collection. Feedback from key-informants and interviewers’ experiences resulted in minor modification in interview behavior, slight revision of wording to equate meaning across cultures, and removal of one item from the demographic sheet. For example, identification of clan membership was removed from the demographics protocol after the first interview conducted in MN. The question was not culturally appropriate and created unnecessary potential for tension. We removed this question based on lack of necessity for the information and respect for participants’ rights. All qualitative data collection materials are available for review in Appendix C.
Data analysis
Data analysis was iterative and participatory in nature, beginning during data collection. The research teams met regularly during qualitative data collection to listen to interviews, discuss narratives and emergent themes, and develop the codebook for data analysis. Two trained research assistants transcribed all interviews into an electronic Microsoft Word document, removing all identifying information from the transcript. The lead researcher reviewed all transcripts while listening to the audio recordings; correcting errors and seeking consultation from the research team when struggling to differentiate content. After transcriptions were complete, they were uploaded into NVivo qualitative data analysis software, and subjected to thematic coding procedures to identify major themes in the data related to the research questions:
- How do “resilient” Somali refugees living in the US conceptualize resilience?
- What resources contribute to resilience processes and outcomes, across contexts?
- How does context and culture shape descriptions of health and well-being?
Codebook development
Following procedures described by MacQueen, McLellan, and Milstein (1998), a structured codebook was developed using a team-based approach. According to MacQueen et al. “the codebook functions as a frame or boundary that the analyst constructs in order to systematically map the information terrain of the text” (p. 32) and serves as a framework from which other researchers can understand the analytic process utilized in the study. The codebook provides a way of breaking down the content into much smaller, thematic chunks, adding a mnemonic code that adds meaning to the larger chunks of data. The codebook was created in a Microsoft Word document and included four components: a) a mnemonic code, b) a full definition, c) key words, and d) example passages showing how the code may appear within the text.
As interviews were conducted and transcribed, the research team listened to the interviews and read transcriptions repeatedly, getting close to the data and gaining an understanding of both manifest and latent content. Once all interviews were completed and transcribed, the lead researcher selected two interviews to formally develop the codebook. The transcripts were chosen based on depth and breadth of the interview, location of the interview (one from Minnesota and one from Alaska), and gender of the key-informant (one from a female and one from a male). Each member of the research team read the selected transcripts. We generated codes (or code names representing common themes) based on the transcripts and previous notes and discussions that occurred during data collection.
We generated three codebooks to apply in three-waves of coding. The first two codebooks were strictly theoretical. We coded broadly into the three broad contexts of Somalia, refugee camp, and US. Next, we coded broadly into individual, relational, communal, and cultural codes. Finally, we applied the collaboratively developed, emergent theme codebook, which allowed for a concentrated evaluation of navigation for and negotiation of health sustaining resources and indigenous pathways to resilience across contexts. The final codebooks were reviewed and verified by cultural advisors. All three codebooks can be viewed in Appendix D.
Coding and analysis
Once all interviews were complete and the codebook was developed and verified by our cultural advisors, data coding began. The lead researcher accomplished the first wave of coding by broadly categorizing data into the context in which the answer referred (Somalia, refugee camp, US). These three contexts were specifically prompted for during the interviews to capture contextual similarities and differences and to facilitate later broad contextual comparisons in the data (between the Somalia, refugee camp, and the US contexts). A second coder reviewed coding for accuracy based on collaboratively defined coding definition. These three codes (as well as a ‘nuanced context’ code that was applied during the second wave of coding) were merged into a broad level titled ‘context.’.
The second wave of coding was aimed at categorizing data according to a systemic model of resilience to help facilitate integration of qualitative and quantitative findings. Specifically, five broad codes were applied to all transcripts to categorize data thematically by context (here a ‘nuanced context’ code was applied and later merged into the broader context variable encompassing all context codes), culture, community, family and individual factors. One transcript was selected by the lead researcher and coded by two independent coders (the lead researcher and a research assistant) in order to calibrate inter-rater reliability. The researchers met and discussed the coding process and discrepancies until reliability was close to 90% as measured by the Kappa statistic. This Kappa is considered within the range of excellent agreement (Fleiss, Levin, & Paik, 2003).
Once inter-rater reliability was established, the lead researcher coded the remaining transcripts using the agreed upon coding scheme. The second coder independently coded every third transcript, meeting with the lead researcher to review their codes, discuss coding discrepancies, and revise the codebook as needed. Prior to these meetings, the two NVivo files were merged, allowing the coding team to identify disagreements in coding quickly and efficiently and to calculate Kappa coefficients. Coders settled coding discrepancies by reviewing whether a code was applied appropriately or applied inappropriately. If the coding team could not agree on a resolution, the text was annotated and resolved in collaboration with the research team and cultural advisors. The lead researcher recoded the portions of text applying the revised codebook as revisions occurred.
The third wave of coding involved the application of codes that emerged from the data. The coding process was iterative, shifting between coding and analysis, eventually arriving at a condensed set of overarching themes related to resilience in the Somali refugee context. From these overarching themes, and in collaboration with the cultural advisors, the research team answered the broad research question, “How is resilience conceptualized according to Somali culture and in the context of forced displacement?” Specifically, the research team defined and/or identified the following terms/items: Health (and well-being)? What are health-sustaining resources? How are health sustaining resources (and feelings of health and well-being) navigated and negotiated for in the context of Somali culture and forced displacement? Kappa statistic estimated reliability close to 90% for this third wave of coding as well and cultural advisors provided a credibility check during this phase of coding (Morrow, 2005). The qualitative results of phase one are presented in Chapter Four.
Phase Two: Selection, Translation, and Back-translation of Study Measures
The following measures were selected based on consultation with cultural advisors (Personal Well-being Index-Adult, PWI-A) and/or qualitative data findings Meaning in Life Questionnaire (MLQ). Post-migration life difficulties (Post-migration Living Difficulties, PMLD) were measured as a way of statistically examining impact of post-migration adversity. The Resilience Research Center-Adult Resilience Measure (RRC-ARM), of course, measured resilience. The selected measures are described in more detail below, under the section titled “Phase Three Measures.”
To ensure semantic equivalency, we engaged the process of translation and back-translation iteratively (Brislin, 1970) and developed a quantitative survey of resilience. Language Translation Services (LTS) – a company that specializes in providing translation and interpretation services to Somalis in the US – along with cultural advisors, worked carefully to adapt study measures.
First, LTS translated the study measures (PWI-A, MLQ-9, and RRC-ARM) into Somali. A Somali version of the PMLD already exists and, thus, there was no need to translate this measure. Next, a second translator back-translated the Somali version into English without access to the original measure. Third, the English translation was compared to the original English version. Based on discrepancy of meaning between some items on each measure, one cultural advisor revised the Somali translation, focusing on meaning equivalence. We repeated the process, starting at step two. After two iterations, the research team deemed the measures “equivalent” and submitted the measures for review to cultural advisors (“verifiers”).
Cultural advisors provided final verification of study measures. We emailed the study measures, description of the translation goals, and instructions for item-by-item checking to two cultural advisors. They read each item of the measure in English and Somali (items were provided in English and Somali on the same sheet of paper, simplifying the verification process) and rated the item in two domains: clarity of translation and meaning equivalence. The verifiers submitted their ratings to the lead researcher. Minor revisions occurred based on review and cultural equivalence was agreed upon across the group.
Phase Three: Quantitative Data Collection and Analysis
A quantitative phase was implemented to develop a resilience measure psychometrically for Somali refugees, and further evaluate resilience and its interrelationships with other study variables. We administered a survey of life difficulties, resilience, personal well-being, and meaning in life to a sample of Somali people living in the US (n = 137). We explored the factor structure of RRC-ARM and evaluated reliability, construct validity, and incremental validity of the measure. Specifically, we sought to answer the following research questions:
- What kind of factor structure can be established for a measure of resilience among Somali refugees?
- Can enough evidence be produced to support the reliability of the RRC-ARM?
- Can enough evidence be produced to support the construct validity of the RRC-ARM?
- Can enough evidence be produced to support the incremental validity of the RRC-ARM?
Sampling and recruitment
Participants were recruited through online media (i.e., through Facebook, Twitter, and email listservs) and community organizations in Minnesota and Alaska. Based on the subject-to-variable ratio that suggests recruiting at least five times the participants as variables on the measure subjected to exploratory factor analysis (i.e., the 27-item RRC-ARM), a minimum of 135 participants were sought for the study (Bryant & Yarnold, 2000). The study was advertised at community agencies in Minnesota and Alaska via advertisements (in English and Somali), newspaper advertisements, on Facebook, and through word-of-mouth recruitment.
Participants
One hundred thirty seven participants completed the Somali Resilience Project survey. Most participants lived in Minnesota (n = 109), followed by Alaska (n = 14), and a scattering of other participant spread across the US who were recruited through methods described below. Participants ranged in age from 18-67 (M = 32.47, SD = 12.52) with slightly more women (51.1%) than men completing the survey. Nearly all participants identified as Muslim. Most of the sample was single (48.9%), followed by married (38.8%). Participants lived in refugee camps for an average of 4.52 years (SD = 5.93; range = 0-19) before resettling in the US. The average number of years living in the US was 10.04 years (SD = 5.93; range = 1-33). Most participants (80.9%) completed hardcopy surveys (80.9%) without the assistance of an interpreter (64.2%). The complete demographic profile of phase three participants is presented in Table 3.
| Table 3
Phase Three Demographic Profile |
||
| Variable | N | % |
| Method of Administration | ||
| Online | 26 | 19.1 |
| Paper | 110 | 80.9 |
| Interpreter Administered | ||
| Yes | 22 | 16.2 |
| No | 88 | 64.2 |
| Not sure | 26 | 19.1 |
| State of Residence | ||
| Minnesota | 109 | 79.9 |
| Alaska | 14 | 10.2 |
| Other | 14 | 10.2 |
| Gender | ||
| Male | 60 | 43.8 |
| Female | 70 | 51.1 |
| Highest Level of Education | ||
| Less than high school | 19 | 14.3 |
| High school/GED | 16 | 12.0 |
| Some college | 28 | 21.1 |
| 2-year degree (associates) | 17 | 12.8 |
| 4-year degree (BA, BS) | 38 | 28.6 |
| Master’s Degree | 15 | 11.3 |
| Religious Faith | ||
| Muslim | 131 | 98.5 |
| Total Household Income | ||
| Less than $10,000 | 40 | 29.9 |
| $10,000-19,999 | 28 | 20.9 |
| $20,000-29,999 | 27 | 20.1 |
| $30,000-39,999 | 18 | 13.4 |
| $40,000-49,999 | 4 | 3.0 |
| $50,000-59,999 | 4 | 3.0 |
| $60,000-69,999 | 2 | 1.5 |
| $70,000-79,999 | 4 | 3.0 |
| $80,000-89,999 | 3 | 2.0 |
| $90,000-99,999 | 1 | 0.7 |
| $100,000 and above | 3 | 2.0 |
| Marital Status | ||
| Married | 52 | 38.8 |
| Single | 67 | 48.9 |
| Separated, Divorced, Widowed | 15 | 11.2 |
Data collection procedures
The study was available nationwide online and in pen-and-paper format in Anchorage and Minneapolis. All forms were identical in content. Participants who elected to participate online followed a link to an online survey. They were prompted to review and sign consent form electronically that overviewed confidentiality, risks/benefits, compensation, and issues of voluntary participation. The online survey began with collection of demographic information from the participant (i.e., age, gender, marital status, religious orientation, annual personal and household income, nationality, refugee status, number of years in the US, length of stay in refugee camps, location of camp). Following collection of demographic information, participants completed the study measures (RRC-ARM, PMLD, PWI-A, and MLQ-9).
Participants who elected to participate via pen-and-paper followed the same procedures as online, but a staff member at the community program explained the study to interested participants and offered a survey in an addressed and stamped envelope. Participants who were unable to read or write Somali or English had the option to participate in the study orally at several community locations. Twenty-two participants completed the study through an interpreter. In all cases, the study took about 20 minutes to complete and interested participants were entered into a drawing for one of six $50 cash prizes.
Measures
Several measures were administered during phase three data collection. Each measure is described in detail below.
Resilience Research Centre- Adult Resilience Measure (RRC-ARM)
Study participants completed the 27-item Somali language version Resilience Research Center- Adult Resilience Measure (RRC-ARM). The RRC-ARM was adapted from the Child and Youth Resilience Measure (CYRM; Liebenberg, 2011, personal communication).
The CYRM was designed as a “screening tool to explore resources (individual, relational, communal, and cultural) available to youth aged 12 to 23 years old, that may bolster their resilience” (Liebenberg & Ungar, 2009, p. 2). The IRP developed the CYRM collaboratively with 14 research sites in 11 countries around the world (i.e., Sheshatshiu, Labrador; Halifax, Nova Scotia; Winnipeg, Manitoba; Hong Kong, China; Medellin, Colombia; Tampa, Florida; Banjul, The Gambia; Imphal, India; Tel Aviv, Israel; East Jerusalem, Palestinian Occupied Territories; Moscow, Russia; Cape Town, South Africa; and Moshi, Tanzania). These sites were chosen for the diversity each would bring to understanding resilience among children living in high-risk environments (Ungar, Liebenberg, et al., 2008). Results of a multi-national validation study suggest the CYRM is a reliable measure of resilience, with items relating to one another as hypothesized in an ecological model (individual, relational, communal, and cultural). The measure demonstrated good reliability at each level of the model (Cronbach’s alphas .84, .66, .79, and .71, respectively).
Colleagues of Liebenberg adapted the CYRM for use with adult populations (personal communication, Liebenberg, 2011). The data produced by this study are the first to evaluate the psychometric qualities of the RRC-ARM and explore the factor structure of the measure when administered to Somali refugees living in the US. Participants were asked to rate their level of agreement with each item of the RRC-ARM on a scale from 1 (not at all) to 5 (a lot). RRC-ARM total scores were obtained by adding all 27 items of the measure; subscale scores were obtained by summing each item belonging to the scale. Higher numbers equate to greater resilience.
Personal Well-being Inventory- Adult Version (PWI-A)
Study participants completed the 9-item Somali language version of the Personal Well-being Index-Adult (PWI-A). The PWI-A was developed to measure subjective well-being through questions related to satisfaction with specific life domains. The measure contains eight items of satisfaction, each corresponding to a quality of life domain (i.e., standard of living, health, achieving in life, relationships, safety, community-connectedness, future security, and spirituality/religion). These eight domains are theoretically embedded, as representing the global question: “How satisfied are you with your life as a whole?”
Cummins, Eckersley, Pallant, van Vugt, and Misajon (2003) reported cumulative psychometric characteristics of the PWI-A, and detailed data on scale composition, reliability, validity, and sensitivity are available in the many reports provided on the Australian Unity Well-being Index (http://www.deakin.edu.au/research/acqol/index_well-being/index.htm) and other countries (e.g., Lau, Cummins, & McPherson, 2005; Tiliouine, 2006). The measure demonstrates good reliability in cross-cultural studies, with Cronbach’s alpha ranging from .70 to .85. Interdomain correlations are often moderate (.30-.55), and item-total correlations are at least .50. The index has also demonstrated good test-retest reliability across 1-2 week intervals with an intraclass correlation coefficient of .85 (Lau et al., 2005).
Participants were asked to rate each item of the PWI-A on a scale of 0 (Completely Dissatisfied) to 10 (Completely Satisfied). Overall PWI-A scores were averaged by summing all nine core items of the measure and dividing by nine. Higher numbers equate to greater personal well-being. The current sample produced a Cronbach’s alpha = .96 on the PWI-A.
Post-migration Living Difficulties Questionnaire (PMLD)
Study participants completed the Somali language version of the PMLD, a 24-item questionnaire developed by Steel and colleagues (1999) based on discussions with a range of legal workers and cultural advisors working with refugee and asylee communities. The questionnaire was developed to assess common difficulties related to the post-migration experience and has been applied with a variety of refugee populations (e.g., Momartin et al., 2006). Bentley (2011) recently adapted the questionnaire for use with Somali refugee populations and provided a copy for use in this study.
The PMLD asks participants to rate their level of experience with a series of common difficulties following forced-migration on a scale from 1 (No problem at all) to 5 (A very serious problem). Overall PMLD scores were calculated by summing all items of the measure and dividing by nine. Higher numbers equate to greater post-migration life difficulties. A higher number equates to greater post-migration difficulty. The current sample produced a Cronbach’s alpha = .90 on the PMLD.
Meaning in Life Questionnaire (MLQ)
Participants completed the 10-item Somali language version of the Meaning in Life Questionnaire (MLQ; Steger, Frazier, Oishi, & Kaler, 2006). Steger and colleagues developed the measure in response to the need for a concise, valid measure of the construct. They defined meaning in life as “…the sense made of, and significance felt regarding, the nature of one’s being and existence” (p. 81). The measure consists of two, 5-item subscales assessing the presence of meaning in life and the search for meaning in life.
The MLQ was developed based on subjective, constructivist perspectives on meaning in life. Original development and validation involved generation of 84 items specifically designed to capture presence of meaning in life and search for meaning in life. A team of researchers evaluated the items based on the aforementioned criteria and retained 44 items. Steger and colleagues (2006) conducted a series of studies aimed at exploring reliability and validity and refining the measure for parsimony and psychometric integrity.
In the first study (1a), they administered the 44-item measure to a sample of undergraduate students (n = 151). Data were subjected to exploratory factor analysis. Two factors emerged and seventeen items were retained. Next (1b) they administered the 17-item measure to a sample of undergraduate students (n = 154). Data were subjected to confirmatory factor analysis to further refine the item pool resulting in the 10-item MLQ. They demonstrated good internal consistency for Presence and Search subscales (.86 and .87, respectively). Moreover, they demonstrated theoretically-expected convergence with and discrimination from other measures. In the second study, they sought to replicate their findings in an independent sample of 400 undergraduate students. Factor loadings were between .65 and .83 on the intended factors and fit indices suggested good fit of the model to data.
Steger et al.’s (2006) third study was aimed at further establishing convergent and discriminant validity of MLQ subscales and compares discriminant validity to other measures of life meaning. Convergent validity and discriminant validity were demonstrated for both MLQ subscales. The MLQ-P demonstrated better discriminant validity than two other commonly used meaning measures. The MLQ has been translated into many languages and validated across many cultures and is widely considered a clean, direct, robust and face valid measure of meaning in life. A search of published literature suggests that it has never been administered to a Somali sample until now.
In the present study, participants were asked to rate their level of agreement with each item of the MLQ on a scale from 1 (absolutely untrue) to 7 (absolutely true). MLQ subscale scores were obtained by adding each item belonging to the subscale and dividing by the total number of items on the subscale. Higher numbers equated to greater presence or search for meaning. The current sample obtained Cronbach’s alphas of .91 (presence) and .87 (search) on the MLQ. Phase three data collection materials are all available for review in Appendix E.
Data analysis
Data analysis was conducted to examine the internal structure of the RRC-ARM and its external relationships with other study measures. These analyses documented information on reliability, validity, and factor structure of the measure when administered to a Somali refugee sample.
Internal structure of the RRC-ARM
The internal structure of the RRC-ARM was examined first through an exploratory factor analysis of the measure and then by standard reliability analyses.
Exploratory factor analysis (EFA) was used to investigate the underlying factor structure of the RRC-ARM with no preconceived notion or theory placed on the data. Kaiser’s stopping rule (1960, as cited in Bryant & Yarnold, 1996) was applied; thus, only factors with eigenvalues of at least 1.00 were retained in the analysis, and a scree-test was conducted to help determine the appropriate number of factors to retain (Stevens, 1986, as cited in Bryant & Yarnold, 1996). Based on previous research (Liebenberg, Ungar, & Van de Vijver, 2012; Ungar & Liebenberg, 2011), the factors were expected to correlate with one another. Therefore, factors were subjected to an oblique rotation in an attempt to achieve a simple structure, thus aiding in interpretation of the analysis (Bryant & Yarnold, 1996). The factor loadings on each item were examined and items with no loading above .40 on any factor were removed, as were items that loaded highly on more than one factor.
For the purpose of this dissertation, RRC-ARM scores were calculated in two ways. First, participant scores on the Somali RRC-ARM were calculated by adding together raw scores to create a total resilience score. Subscale scores were then calculated by adding together the items that loaded on each factor. Participant scores were also calculated by weighing the Somali RRC-ARM items based on their factor loadings. The weighted items were then added together to create a total score, and subscale scores were calculated by adding together the weighted scores on the items that loaded on each factor. All analyses were conducted using both sets of Somali RRC-ARM scores.
Reliability and validity of the Somali RRC-ARM
Internal consistency of the Somali RRC-ARM was explored by calculating Cronbach’s alpha for the overall scales, for each of the factors revealed by the EFA, and by examining intra-factor and inter-factor correlations.
Convergent validity was examined with a series of bivariate correlations to explore theoretically expected relationships between the Somali RRC-ARM and other study variables. Incremental validity (or clinical utility) was examined through hierarchical regression analyses.
A first set of Pearson correlation analyses was conducted between the Somali RRC-ARM and the PWI-A to test the hypothesis that resilience (as measured by the entire Somali RRC-ARM, as well as the subscales that emerge) would positively correlate with personal well-being (as measured by the PWI-A).
A second set of Pearson correlation analyses was conducted between the Somali RRC-ARM and the PMLD to test the hypothesis that resilience (as measured by the entire Somali RRC-ARM, as well as the subscales that emerge) would be negatively correlated with systemic difficulties related to the post-migration resettlement experience (as measured by the PMLD).
A third set of Pearson correlation analyses was conducted between the Somali RRC-ARM and the MLQ to test the hypothesis that resilience (as measured by the entire Somali RRC-ARM, as well as the subscales that emerge) would positively correlate with presence of life meaning and purpose (as measured by the ‘presence of meaning’ subscale of the MLQ).
Bivariate correlations were conducted between well-being (as measured by the PWI-A) and status variables (i.e., age, length of time living in the US, level of education, marital status, and income) that should be related to personal well-being theoretically. A series of hierarchical regression analyses were then conducted to test the hypothesis that resilience (as measured by the Somali RRC-ARM) would account for variance in personal well-being (as measured by the PWI-A) above and beyond the contributions of post-migration living difficulties (as measured by the PMLD), presence of life meaning (as measured by the ‘presence of meaning’ subscale of the MLQ), and other status variables related to personal well-being. The total personal well-being score of the PWI-A was entered as the outcome variable. The predictor variables were entered in a stepwise fashion, starting with status variables in the first step, then the PMLD in the second step, then the ‘presence of meaning’ subscale of the MLQ in the third step, and the Somali RRC-ARM (total score) in the fourth and final step.
Hunsley and Meyer (2003) argued that a hierarchical regression is one way to demonstrate a measure’s incremental validity. They argued that a statistically significant unique contribution of a scale after it was entered on at least the third step of a regression analysis is a good indicator of its incremental validity and clinical utility. Because r increments become generally small by the third step of a regression equation (Nunnally & Bernstein, 1994), Hunsley and Meyer (2003) proposed that a semipartial r of .15 to .20 on the third step indicates good incremental validity and clinical utility of a measure. A contribution of the magnitude that Hunsley and Meyer (2003) suggested on the third step of a regression takes into account variance that is likely to be shared by all three predictor variables. In this regression analysis, a semipartial r that is close to or above Hunsley and Meyer’s (2003) recommended benchmark of .15 by the third step (because the RRC-ARM will be entered in the third step), or at least equal to Cohen’s (1992) recommended benchmark of .10, will be considered a good indicator of incremental validity.
Chapter 4: Qualitative Findings
The purpose of phase one data collection was to gather information about resilience (i.e., the experience of health and well-being in the context of adversity, the resources that support these experiences, and the process of navigating the context toward health-sustaining resources). In this chapter, the qualitative findings from phase one are presented in the following order: a) contextual description of adverse experiences; b) health-sustaining resources; c) individual experiences; d) family culture and relational networks; and e) Islamic beliefs and meaning in life.
Context of Adversity
My family lived in Mogadishu. We lived a really good life, and then in a blink of an eye everything was taken away. I remember coming home from school and eating lunch before we go to Islamic school. I was playing in the front yard and my family tells us we have to flee. Just like that, we leave our entire life behind.
Participants described experiences of adversity across three broad contexts: a) in Somalia after the onset of the Civil War; b) while living in refugee camps; and c) after resettlement in the US. Exposure to physical and sexual violence, death of loved ones, harsh environmental conditions, lack of food and water, acculturation stress, and discrimination emerged differentially across contexts as the most common forms of adversity.
Somalia
Key-informants described a peaceful lifestyle in Somalia prior to the onset of Civil War. Strong family culture, broad relational networks, and collective resource sharing contributed to thriving communities and life satisfaction. Islamic religious practices produced the rhythm of day-to-day activities, and poets entertained by crafting spoken word into prose exemplifying cultural values and traditional knowledge. According to key-informants, life changed in an instant for Somali people living in Mogadishu and southern regions of the country in the early 1990s. Clan-based violence ripped through communities, disrupting family culture and relational networks. Warlords restricted access to health-sustaining resources, such as food and water, and collective resource sharing fell to the whim of those in power. Exposure to physical and sexual violence, and death of loved ones emerged as the most common forms of adversity after the onset of war in Somalia.
One key-informant shared: “There was no government in Somalia. There were rebels killing everybody. Raping, looting, and killing innocent people. Women were raped and villages invaded every day. It’s a very, very hard life to live.” And another key-informant shared: “My brothers and sisters, some of them die. One died in front of us. I remember everywhere was artillery and gun fire. I run to the bush and say, ‘which way do I go, which way is Kenya?’”
Key-informants portrayed a long, dangerous migration away from Somalia, toward refuge in neighboring Kenya. Families were often separated during escape; some were never reunited. Refugees typically traveled by foot carrying what belongings they had on their backs. Exposure to physical and sexual violence, harsh environmental conditions, and hunger emerged as the most common forms of adversity during migration to Kenya.
Refugee camps
Somali refugees settled in refugee camps inside the border of Kenya. Displaced persons quickly overwhelmed the camps. Access to resources was limited, and quality of life was low. Exposure to physical and sexual violence, and lack of food and water, emerged as the most common forms of adversity while living in refugee camps. Several women described struggling to feed their children who were malnourished after the journey from Somalia.
We just try to feed the children whatever we have to cook. We have to go to the jungle to find it and cook for them. There’s no running water. We have to go early in the morning and go in line for water. It’s really harsh, tough life.
Safety remained an issue in refugee camps. Clan-based violence followed refugees into camps “There are people every day being shot by Somali rebels looking for someone. We have a tribal problem. That’s why the war started.” Participants described corruption among the Kenyan military and lack of protection for women and children. One key-informant shared:
The mothers worry about their children getting raped. There are Somali men who rape you, and Sudanese men right there waiting…so it’s scary. You cannot let your girl go away for one second.
Participants had all come to the US as a refugee. They described their process of navigating the refugee aid agencies and the United Nations applications and clearance. Once living in the US, a new form of adversity emerged in the form of acculturation stress.
Acculturation stress in the US
Communication difficulties emerged as the most frequent difficulty described by key-informants, followed by difficulty adjusting to the pace of life in the US and difficulty integrating religious practices into the structure of daily life. Ethnic discrimination was noted too. Loss of status once in the US, challenges with practicing Islamic traditions, and difficulty finding employment emerged other acculturation stressors.
One highly educated participant shared her experience coming to the US:
At first, I needed guidance like a 2-year-old. Everything is big, everything is fast, and everything is different. The culture, the weather, and the language—everything is different! Where do you start? You have children sitting there, looking at you, and you don’t even know where to start. I couldn’t communicate, no transportation!
And another participant described difficulty adjusting to the pace of life in the US:
In the United States, the concept of pressure of time and the speed of life is something that I still, even as a professional and an educator, I just cannot catch up with. I can say 80% of my appointments I’m late to them up to now. Regardless of having a schedule and writing it down. That’s a real challenge.
Several key-informants noted difficulty integrating Islamic practices into life in the US. They described hesitance to engage in prayer during work hours, and distress when they were unable to engage in their religious practice. One key-informant shared:
Cultural expectations and social norms are different for somebody coming from conservative, traditional life in Somalia. Now we have to operate in a multi-cultural, multi-ethnic community. How do you practice your religion when you’re in the middle of a meeting and prayer time comes? Although in a way the US system is very open and accommodating, especially in Minnesota, you still have people who are not aware and think that you take things for granted when you break for prayer. You must find courage or suffer the consequence of missing prayer.
Finally, discrimination emerged as a common form of adversity faced in the US. Key-informants described people staring at them in public places and making derogatory comments regarding their clothing and religious beliefs. Several key-informants described an increase in discrimination following the September 11, 2001 terrorist attacks. For example, one key-informant shared:
I feel like at times I’ve been discriminated against for who I am, and that’s Somali. After September 11, we went through a lot of challenge in the United States. I mean you can’t walk alone in the streets, and if you do you will be openly discriminated against. There was a time that we went into one of the malls and the employees discriminated saying that, ‘Oh, you Bin Laden’s daughters or wife, what are you doing here? Go back to your church’, and all this. It still happens. You know, people tend to kind of use what they see on TV or on the news.
In sum, the form of adversity (acute stress, chronic stress, environmental stress, etc.) varied by context. Participants described exposure to physical and sexual violence, death of loved ones, exposure to harsh environmental conditions, and lack of food and water as the most commonly experienced forms of adversity in Somalia and in refugee camps historically and presently. Chronic acculturation stress and ethnic discrimination emerged as a primary form of adversity experienced in the US.
The Post-migration Living Difficulties Measure (PMLD) was chosen as a measure for phase three data collection. The PMLD captures information about exposure to stress and life difficulty common among refugee populations. The PMLD was predicted to correlate negatively with Personal Well-being and resilience.
Health-Sustaining Resources
Physiological needs (i.e., food and water) emerged as foundational health-sustaining resources without which other resources were not of concern. Only slightly less emergent than food and water, was shelter and safety. Opportunity for employment and education were both facilitators of access to health-sustaining resources and valued life directions in Somali cultural experience.
Basic needs
Key-informants described limited access to food and water during forced migration and some described malnutrition and death: “There is really bad malnutrition. You see children malnourished, adults dying. Nobody can take care of them.” Access to food and water increased once living in refugee camps; however, these resources remained scarce. Shelters in refugee camps were fashioned of tarps and other materials provided by the United Nations. While these shelters offered protection from harsh environmental conditions (“The houses are tents made of a huge blue plastic thing over head to protect from the rain and things like that.”), they did little to secure the safety of refugees. The general consensus among key-informants was once basic needs were met, refugees considered how to improve their situation.
When we were living in Kenya, among the refugee camps, we start to think, how do we get out of this situation that we are in? Even though we had some safety, we didn’t have enough safety to stay. Kenya was only a little bit better than Somalia.
Education and employment
Key-informants described efforts to generate income while living in refugee camps. According to one key-informant: “Somalis are so good at running business. They are really hard working and they know how to make money.” Men and women both contribute substantially to generation of financial resources. According to key-informants, access to educational and employment opportunities support one’s ability to not only fulfill basic needs and secure shelter and safety, but also to contribute to broader family systems and relational networks.
Key-informants described efforts to generate income by working within the camps, helping to distribute goods and perform other essential services, or digging latrines. Some refugees migrated to Nairobi to purchase health-sustaining resources (e.g., clothing) and then sell the goods in refugee camps. One key-informant described how this effort not only generated income for the individual (and family), but also provided for the broader community within the camp.
Once in the US, access to basic needs, shelter, and general sense of safety increased substantially. Key-informants described turning attention to educational and employment opportunities. Gaining employment was difficult for many key-informants. Lack of employment experience in the US, loss of worth of education, and communication difficulties contributed to struggles to obtain employment. Despite these challenges, all key-informants eventually secured employment by applying their skills and qualifications in a variety of ways. Some became interpreters, others became childcare providers, and others assumed roles within social service agencies.
Education was identified as highly valued and as an essential health-sustaining resource across contexts. The form education took differed according to context. For example, those living a nomadic lifestyle in Somalia described an apprenticeship model of education that led to the assumption of important roles in the community, while others living a more contemporary lifestyle described an education system similar to that common in the US. Education was not only discussed as a valued health-sustaining resource, but also a facilitator of access to additional health-sustaining resources needed to raise a family and contribute to the community.
In sum, health-sustaining resources emerged in a hierarchy of needs (Maslow, 1943). Water, food, shelter, and safety emerged as baseline health-sustaining resources. Once basic needs were met, education and employment opportunities emerged as culturally valued and contextually relevant health-sustaining resources. Key-informants described how generating income allows contribution of resources to family and other relations. A key-informant explained how sharing resources is highly valued in Somali culture and contribute meaningfully to the broader family system and community relationships.
Partly because of these qualitative findings, the Personal Well-being Inventory (PWI-A) was chosen as a measure for phase three data collection. The PWI-A captures information about subjective well-being across several domains, including: standard of living, health, personal achievement, interpersonal relationships, sense of safety, community belonging, future security, and spirituality or religion. The PWI-A was predicted to correlate positively with resilience (Somali RRC-ARM) and meaning in life (MLQ), and correlate negatively with post-migration living difficulties (PMLD).
Health and Well-being
Health all goes under spirituality. To keep healthy mentally, to keep healthy emotionally, to keep health physically, you must have a strong Iman [faith], and pray. If you do that, emotionally, mentally, physically, you will be taken care.
Participants described health holistically. Commitment to spiritual faith and religious practices, freedom from physical and mental illness, production of a healthful family system, ability to contribute to the family and broader community, all emerged as indicators of health and well-being. Spiritual health, the pinnacle from which other expressions of health emerged, included strong resonance with the term Insha Allah.
One key-informant shared the following words: “Insha Allah. To God we belong and to Him we’ll return. Something good will come out of all life experiences.” He described how Islamic faith and religious practice has shaped Somali culture for thousands of years.
Making meaning of life experiences and finding purpose in life is prescriptive of Islamic practice and represents a form of existential resilience. It is within this cultural context that resilience is experienced. Thus, the Meaning in Life Questionnaire (MLQ) was chosen as a measure for phase three data collection. The MLQ captures information about presence of meaning in life and search for meaning in life. The MLQ was predicted to correlate positively with resilience (RRC-ARM) and personal well-being (PWI-A).
Individual Experience
Every society has people who are very successful and very determined. They have the drive to be successful. And there are some people who don’t have the drive, who don’t have the ambition. No matter where you are at, whether you are in a refugee camp, whether you’re in United States, or whether you are back home, determination is the key for your future.
Individual capacity contributes to one’s ability to effectively navigate toward, and negotiate for, health-sustaining resources (i.e., food, water, safety, security, material resources, and education). Key-informants described resilient Somali people as determined, hardworking, assertive, future-oriented, and goal driven. These traits were described in direct relation to one’s ability to contribute to the broader family system through the generation of health-sustaining resources.
Determination
According to key-informants, determination varies from individual to individual and, in many ways, defines resilience at the individual level. This culturally valued trait was considered as universal and cross-contextually important. When asked to explain what a Somali person needs to live well, one key-informant shared:
Oh, it’s to be determined. Sometimes you going to be bumped down, but you have to bounce back. For example, when I finish my college [in Somalia], I have to take a test for job placement. They were looking for only 15 people for malaria control. The man asked me, ‘Why are you here? Who are you with?’ I say, ‘I am one of the people who took the job placement test; I was the highest scoring person’. And he said, ‘I think there is a mistake, you need to go back to human resources, because we never hire a female before’. I say, ‘don’t tell me what I don’t deserve, what I can do, what I cannot do.’ So I went there and I fight for 6 months, every day, never stopped. It was paid back! I was so excited. I was the first woman to be hired there. I show woman can do what man can do. I was determined I could do that. I put my head to it and follow through.
This focus on determination was common throughout the resilience narratives. Determination was closely related to assertiveness, a trait that contributes to well-being across contexts, and seemed especially pertinent to accessing resettlement resources in refugee camps. For example, one woman described her efforts to hasten resettlement for her family and community through assertiveness and advocacy:
After we come to the camp, we file the paperwork and the sponsorship and everything and we just waiting to get an answer. We never informed of anything. So I write to the director of the organization. I say, ‘I think people who come after us have been responded to already. I’m wondering what is going on. My family has been separated by this war and this trouble. We rely on you. We are in a refugee camp, we are not in a good place, and we are not in good shape. We are looking every day, wondering who is going to respond to us. Please take this very seriously. People are struggling here and hoping to get out. Their family’s been separated and they want to come together. Please take your job serious.’ She responds with invitation for a screening. I am amazed! She changed as soon as I communicate this way. This is the reason I am here. There is a Somali saying, ‘If you don’t speak, even your mom will forget you.’ You have to speak up.
In this example, determination and assertiveness contributed to the hastening of the resettlement process. The ability to read and write, however, also contributed to the process. The key-informant reflected, “If I don’t know how to write, maybe never respond to us.”
Functioning skill sets emerged as important contributors to resilience across contexts. In the context of a nomadic lifestyle in rural Somalia, accessing health-sustaining resources (e.g., food, water) through nomadic migration required a specific skill set learned through an apprenticeship model of education. In refugee camps, knowledge of food sources and cooking skills were essential to survival, as were important business skills and comfort with migration between locations, as this led to the ability to travel, purchase, and sell goods in the camp. Literacy, often gained through formal education systems in Somalia, contributed to the ability to navigate the resettlement system and gain access to health-sustaining resources once resettled in the US. English-language ability emerged as an essential skill related to resilience once in the US. One key-informant shared:
To be a successful person you have to educate yourself; you have to build from the base and go up the ladder. And when I say this, you see, you have to go to school, get a graduate degree, and then get a job. A lot of [Somali] people in America don’t do this because of the language barrier… knowing English is a privilege when you are living in the United States.
According to key-informants, determined individuals were more likely to seek out opportunities for education and employment and were better able to contribute to the family system. One key-informant described how her determination and hard work translated to pride in that she was able to support her family once resettled in the US:
First, I go to second language English school. Then I took a test. I am good at math, and no matter the language, the formula is there. I work my way toward my GED and then started college. Because I really dislike waiting for somebody to support me, I go to school, go into work, sometimes work double shift. I have to do your homework at night. I left home at 8:00 a.m. and come back at 1:00 a.m. I was so excited. I feel so good, so proud because I supporting my family now. And that makes me tireless.
This same key-informant worked tirelessly to support her family in Somalia as well. She explained:
I used to prepare and scrub cars and resell again, or go to pharmaceutical factories and get medicine distributed to pharmacies. Those things I was doing besides my job. I was determined to help support my mother and my father.
Future orientation
In addition to determination, hard work, and assertiveness, key-informants described the presence of hope and a focus on the future as important components of resilience. One key-informant shared a Somali saying: “Why that question being raised: Why?” This quote embodies the cultural norm that overrides the need for answers about the past. As described in detail later, this norm relates to the Islamic faith; however, key-informants shared how resilient individuals express this norm through a tendency to focus on the future, and maintain hope. Another key-informant described the steps he takes when faced with difficulty, he said: “I ask myself: ‘What can I do about this happening? What could I do better? What could I do to prevent next time?’ Those are my questions. It’s not going to be negative, like: ‘Why did this happen?’” This forward focus was evident throughout all of the narratives and translated to specific goals (“As a human being you have to set a goal. Most Somalis have some sort of goal”) as well as more broadly spoken hope for the future versus hopelessness because of the past. One key-informant shared how he focuses on the future and maintains hope each day and views this approach as the key to living well:
I always depend on just looking forward and not looking back on what happened. So that keeps me going and hopeful to a nice bring future for my family, my neighbors, everyone I know. The future is holding a lot and I want to get best of it. I’m hoping always to be the best, very useful person. Every day in your life, when you get up from your bed, that’s hope for the day. Tomorrow is another day. Hope is the key for living. If you’re not hopeful for anything, then you’re nothing, you’re dead.
In sum,individual capacity contributes to one’s ability navigate effectively toward, and negotiate for, health-sustaining resources (i.e., food, water, safety, security, material resources, and education) in the context of adversity. Key-informants described resilient Somali people as determined, hardworking, assertive, future-oriented, and goal driven. These traits were described as important to resilience across contexts. Individual capacity directly impacts one’s perceived level of success in their ability to contribute to the broader family system and thus find their place within the culture.
The RRC-ARM measures individual-level factors that overlap with Somali conceptions presented here. Items include “I cooperate with people around me,” “I try to finish what I start,” “Getting qualifications or skills is important to me,” and “I know how to behave in different social situations.” Cultural advisors felt these items sufficiently captured individual-level factors of resilience and did not recommend adding culturally specific items. Qualitative information contributed to contextual understanding of the individual-level data and informed development of the Somali Multidimensional Model of Resilience.
Family Culture and Relational Networks
“What I know in Somali culture, you have a very strong family. Together we share problems and help each other. When you have a problem you have somebody to lean on. That’s what keeps us going, assurance that if anything happen to you, you have backing from the family.”
Individual capacity can only be understood as an effort to navigate and negotiate for health-sustaining resources to contribute to the broader family system. Family culture emerged as an essential contributor to resilience, and relational networks further support navigation of, and negotiation for, health-sustaining resources. Family provides social and emotional support during times of adversity, and relational networks facilitate access to health-sustaining resources.
Key-informants described family as inseparable from the notion of culture in Somali tradition. The term ‘family’ extends beyond the Western notion of a nuclear family and includes aunts, uncles, cousins, and neighbors. Key-informants described how family members interacted on a daily basis while living in Somalia.
Back home [in Somalia] we have a good family system. My cousins, neighbors, all relate to each other and helping each other. You see everybody, everyday…you see all your relatives, even if you live in separate house. The children took care of each other; the older ones took care of the younger ones. Extended family helped with raising the children.
According to key-informants, meals were prepared collectively, prayer was engaged in together, and family members shared caretaking responsibility. These traditions continue for many Somali people living in the US. One key-informant shared:
I am very close to my family and my family is very close to their other family members. We all practice Muslim faith. Fridays we go to the mosque and pray. We all go, including my children. And the other days we all pray five times a day.
Several key-informants mentioned how the cultural context in the US has challenged some traditional notions of family. For example, one key-informant explained:
I think raising children, family in the US is challenging. Especially trying to convert the culture in Somalia into the United States. I can say the most challenging thing is raising a family here. Having children is important. But raising them is much more expensive and much more challenging.
A generational drift was observed in the family narrative. Older key-informants described challenges associated with integrating Somali family cultural values into the Western value system, while younger key-informants expressed an appreciation for autonomy and challenged the traditional family power structure. For example, a younger woman shared:
Let’s talk about girls my age that live in Somalia right now, or maybe younger than my age. Their life would be tough. Females in Somalia, they don’t have a lot of privilege there. When a girl hits 15 she will be married to an older guy, a family member that her mom and dad approve of. And when a person gets married there, the life is gonna involve their husband and her kids and that’s the future she will have. In Somalia, people don’t have the opportunity to choose their life. No they do not. Over here, I have control over me. My mom doesn’t have control over me. She doesn’t tell me what to do. I can say, ‘this is what I want to do today… tomorrow…this is what I want to accomplish.’
Nevertheless, family culture emerged as an essential component of resilience across contexts. Children are highly valued and contribute to a sense of meaning and purpose in life. One key-informant shared:
To me, my family and my children are what I live for. Every morning that I get up, I worked eight hours; I earn a check. I’m providing for my family, doing what I am supposed to do. To me that is something meaningful. My children, my family, they give me a lot of hope.
In addition to contributing a sense of meaning and purpose in life, family also serves as a conduit of social and emotional support, across contexts. Key-informants described how family members communicate with one another as a problem-solving method. Family collaboration is highly valued when faced with individual challenges. For example, one key-informant shared: “If something bad happens, we sit down as a family and discuss. We go from there and see what we can do to solve the issue.” Another key-informant shared: “The family always cooperate. Somali people, family, they come together during the nighttime. We sit down and talk and we plan.” As family culture transforms in the US, family remains an important component of support and resilience. One key-informant shared:
Support within the family is important. My family, we’re a small family, and most of my extended family is not here. We (family) relate well; we share experiences and take care of the kids and their needs, driving them to places and activities and school. That also makes my life actively engaged and meaningful.
According to key-informants, emotional support typically comes from within the family. One key-informant shared: “There is always somebody you’re so close to, your family, and you can talk to about the way you feel.” Women often mentioned their female relatives (e.g., sisters, aunts, cousins, and mothers) as their primary sources of emotional support. One key-informant shared:
I have a lot of sisters, so I talk to them. I call them and they are my counselors. And also I have a good relationship with my mother, because my mother is a loveable mother. I can share whatever in the life that I want. She is also my helper.
Importantly, emotional support in the form of professional counseling or psychotherapy was described as ‘taboo’. For example, one key-informant shared: “Mental health is an issue that people don’t talk about much. If they do, it is behind closed doors. It is taboo, basically, a taboo… we tend not to share a lot outside the family.”
Collective resource sharing
“There’s a Somali saying: ‘If you are rich, we make you poor. If you are poor, we make you rich.’” This saying embodies the culture of sharing and consideration for the collective needs of the family in addition to individual needs. Consideration of individual needs before collective needs of the family is highly dishonorable. For example, one key-informant explained:
We all share whatever we have in Somalia. If someone doesn’t share we tease that person, say he is greedy and doesn’t take care of the family… doesn’t take care of his relative. We say he’s selfish. Our family system is very close. That’s what helps us to be healthy.
In addition to resource sharing within their local family system, Somali people living in the West share resources (primarily monetary) with family living in Somalia or refugee camps. In fact, some key-informants stated the health and well-being of people living in Somalia and refugee camps today is dependent on resources from family living overseas (e.g., “If they’re living well in Somalia at the moment, they have to have some resource coming to them”). Moreover, family reunification policies favor placement of new refugees with family members living in the US. After resettlement, family members support one another as they resettle, often working toward collective business endeavors.
In sum, individual characteristics such as determination, assertiveness, future-orientation, and functional skill sets help navigation of resources in the context of Somali culture and forced displacement. Family systems and broad relational networks help promote successful navigation of resources across contexts and collective resource sharing promotes health and well-being. The RRC-ARM measures family-relational-level factors such as “My family has usually supported me through life”, “I feel supported by my friends”, “I feel secure when I am with my family”, and “I have opportunities to be useful in life (e.g., caring for others, employment).” Cultural advisors felt these items sufficiently captured family-relational-level factors of resilience and did not recommend adding culturally specific items. Qualitative information contributed to contextual understanding of the family-relational-level data and informed development of the Somali Multidimensional Model of Resilience.
Islamic Beliefs and Existential Resilience
“Insha Allah. To God we belong and to Him we’ll return. Something good will come out of all life experiences.”
Islamic faith emerged as a powerful contributor to resilience across contexts. All key-informants discussedGod’s will as an explanatory model for exposure to life adversity, and religious practices (i.e., prayer) emerged as an emotional coping mechanism. Islamic faith holds that all things happen with purpose (“I believe every step been measured before I born and that happen for that purpose”) and God is the conductor of one’s life path (“Whatever came through to you, it’s already been written”). According to key-informants, each life experience is a test to one’s faith. Hopelessness was described as the antithesis of faith (“Hopelessness is considered negative, the antithesis to one’s faith. There is hope, whatever you go through. Grief is a test.”). One key-informant summarized this concept as follows:
The faith part is always a driving motivator, and provides access to hope. There are some statements in the Quran and the ideas of the prophet Mohammed (peace be upon him) that you should look at those that are in a war situation and those in more difficult situations, regardless of how difficult your situation is, be thankful.
Key-informants described how faith contributes to emotional coping and meaning making in the context of adversity, and how faith allows for forward movement in life (“The concept of God willing keep me on going on”).
Faith is the key component of survival and coping. Because in Islam there is this concept of everything happens by the will of God. So if all these difficulties are happening, it’s like a test for me to try to help and be helpful to others. When you have faith, life is quite different because everything has a different meaning for you. You put everything in God’s hands.
Prayer emerged as a powerful emotional coping mechanism across contexts. Traditionally, Muslim prayer occurs five times a day: at sunrise, noon time, afternoon, sunset, and then again after the sunset. According to key-informants, prayer facilitates connection with God, and contributes to a general sense of well-being, patience, and respectful relations with family members and community. Families gather at the mosque in prayer and meditation, each connecting with a higher power and the greater purpose of life.
While prayer remains an important element of Somali life in the US, challenges with traditional practice emerged in this context. For example, key-informants discussed difficulty arranging their workday to incorporate prayer (e.g., How do you practice your religion when you are in the middle of a meeting and prayer time comes). Others described challenges related to fasting in Northern climates, where daylight is either limited or extended. For example, in Alaska, key-informants described particular challenges with prayer and fasting due to limited daylight in the winter (e.g., “It is difficult to pray all the prayers, five times in four hours”) and extended daylight in the summer (e.g., “Last year, the Ramadan fasting was beginning of August, this year will be July 20. We’re going to be fasting eighteen hours”).
In sum, Islamic faith overarched all aforementioned domains of resilience. The belief in Insha Allah (or God’s will) provides an explanatory model for understanding life adversity. Religious practices (e.g., prayer, reading Quran) emerged as a primary emotional coping mechanism. Islam provides presence of meaning and purpose in the context of adversity and quite possibly contributes the most potent form of resilience among Somali culture.
The RRC-ARM measures cultural-level items that partially assess spiritual resilience. Items include: “Spiritual beliefs are a source of strength for me” and “I participate in organized religious activities.” The MLQ was added due to the poignancy of meaning in life throughout the qualitative narrative of resilience. Meaning in life was predicted to positively correlate with resilience (RRC-RM) and personal well-being (PWI-A). The RRC-ARM was predicted to capture a statistically significant amount of unique variance in personal well-being, above and beyond the presence of meaning in life.
Cultural advisors agreed with the addition of the measure and felt this was a more direct approach to looking at the role of meaning in life and resilience than adding culturally-specific items to the RRC related to meaning in life.
Summary of Qualitative Results
Within this context of adversity (Somali, refugee camp, US), individuals navigate their way toward resources that support health and well-being. Health-sustaining resources emerged in a hierarchy similar to that described by Maslow (Koltko-Rivera, 2006). Physiological needs superseded other important resources, like safety, shelter, and protection from violence. Opportunity (or employment) and education emerged as culturally valued and contextually relevant health-sustaining resources. Opportunity facilitates access to resources and maintenance of basic needs, safety, and security. Contribution to broader family and relational systems is an important component of self-worth. Individual characteristics, such as determination, hard work, and future-orientation contribute to successful navigation and negotiation for health-sustaining resources. Family culture and relational networks support resilience through collective resource sharing and provision of emotional support. Islamic faith provides presence of meaning and purpose in life when faced with life adversity and quite possibly contributes the most potent form of resilience among Somali culture.
Based on phase one findings and collaborative input from cultural advisors, the PWI-A, MLQ, and PMLD were chosen for administration along with the RRC-ARM during phase three of the study.
Chapter 5: Quantitative Findings
The purpose of phase three data collection was to gather quantitative data from Somali people living in the US (n =137) on measures of resilience (RRC-ARM), personal well-being (PWI-A), meaning in life (MLQ), and post-migration living difficulties (PMLD). In this chapter, the quantitative findings from phase three are presented in the following order: a) descriptive statistics and demographic profile of study participants; b) internal structure of the RRC-ARM (factor structure, psychometric evidence); and c) relationship between the RRC-ARM and other study measures (evaluation of convergent and incremental validity).
Data Preparation
Prior to conducting primary data analyses, descriptive statistics were calculated to examine the characteristics of the sample. Descriptive statistics included frequency distributions, means, standard deviations, and ranges for all variables of interest. For the primary data analyses, the RRC-ARM was first subjected to exploratory factor analysis, along with the calculations of various indices that may support the reliability and validity of the measure for Somali refugees. Mean scores were obtained for the RRC-ARM, as well as for each factor that emerged during analysis. For the purpose of this dissertation, weighted factor scores were also calculated for RRC-ARM total scores and factor scores. Mean scores for the other measured variables were also calculated. Finally, a series of bivariate correlations and a hierarchical regression were conducted with the measured variables. The sample’s means and standard deviations on all the measured variables are presented in Table 4.
Table 4
Means and Standard Deviations of Primary Study Variable
| Variable | N | Minimum | Maximum | M | SD |
| Somali RRC-ARM (Unweighted) | 137 | 1.86 | 5.00 | 4.35 | .62 |
| Individual Factor | 137 | 1.83 | 5.00 | 4.42 | .70 |
| Relational Factor | 137 | 1.57 | 5.00 | 4.37 | .73 |
| Cultural Factor | 137 | 1.78 | 5.00 | 4.30 | .71 |
| Somali RRC-ARM (Weighted) | 137 | 1.25 | 3.36 | 2.91 | .42 |
| Individual Factor | 137 | 1.30 | 3.54 | 3.12 | .50 |
| Relational Factor | 137 | 1.09 | 3.60 | 3.14 | .54 |
| Cultural Factor | 137 | 1.05 | 3.05 | 2.59 | .45 |
| Meaning in Life Questionnaire (MLQ) | 134 | 2.30 | 7.00 | 5.28 | 1.03 |
| Presence Subscale (MLQ-P) | 134 | 2.00 | 7.00 | 5.98 | 1.29 |
| Search Subscale (MLQ-S) | 134 | 1.00 | 7.00 | 4.57 | 1.64 |
| Post-migration Living Difficulties (PMLD) | 136 | 1.00 | 4.32 | 1.89 | .71 |
| Personal Well-being Inventory (PWI-A) | 135 | 0.00 | 10.00 | 7.88 | 2.21 |
Note. Participants were asked to rate each item on the Somali Resilience Research Center-Adult Resilience Measure (RRC-ARM) on a scale from 1 (not at all) to 5 (a lot). Mean scores are presented here. Higher numbers equate to greater resilience. Participants were asked to rate their level of agreement with each item of the Meaning in Life Questionnaire (MLQ) on a scale from 1 (absolutely untrue) to 7 (absolutely true). Mean scores are presented here. Higher numbers equated to greater presence or search for meaning. Participants were asked to rate each item on the Post-migration Living Difficulties (PLMD) measure from 1 (not at all) to 5 (a lot). Mean scores are presented here. A higher number equates to greater post-migration difficulty. Participants were asked to rate each item of the Personal Well-being Index-Adult (PWI-A) on a scale of 0 (Completely Dissatisfied) to 10 (Completely Satisfied). Mean scores are presented here. Higher numbers equate to greater personal well-being.
Internal Structure of the RRC-ARM
Exploratory factor analysis of the RRC-ARM
An initial principal-axis factor analysis produced a Kaiser-Meyer-Olkin measure of adequacy of .89, above the recommended value of .60 (Aron, Aron, & Coups, 2009). Bartlett’s test of sphericity was significant, 2 (351) = 2792.32, p < .001. Thus, the assumptions for appropriate evaluation and interpretation of the subsequent factor structure (EFA) of the RRC-ARM were met.
The 27-item RRC-ARM was subjected to an EFA with direct oblimin rotation. This initial EFA produced five factors with eigenvalues greater than 1.00, and this was congruent with the scree-test findings. Thus, two-, three-, four-, and five-factor solutions were explored to locate the most interpretable factor structure. The two-factor solution accounted for 54.6% of variance, had two cross-loading items (items 6, 7), and one-item that did not load highly on either factor. The four-factor solution failed to converge in 25-iterations. The five-factor solution accounted for 69.63% of variance, had two cross-loading items (items 1, 2), and one item that did not load highly on any of the factors (item 19).
Of the four extractions, we chose the three-factor solution. The three-factor solution, which accounted for 61.13% of the variance, was the most interpretable on the basis of theory and the qualitative findings, and this solution produced only one cross-loading item. We dropped that item (i.e., I know my own strengths), along with three items that did not load highly with any factor (i.e., I can solve problems without harming myself or others, I am treated fairly in my community, and I think it is important to support my community) and one item that was theoretically inconsistent with the other items in the factor in which it loaded highly (i.e., If I am hungry, I have money to buy food to eat). Factor 1 (seven items) seems to be tapping into relational or interpersonal contributors to resilience, Factor 2 (six items) seems to be asking about individual level contributors to overall resilience, and Factor 3 (nine items) seems to be related to cultural contributors to overall resilience. These EFA results are consistent with phase one qualitative results at the individual, relational, and cultural levels. The remaining 22 items and their respective factor loadings are presented in Table 5.
Table 5
Three-Factor Correlated Model of the Somali RRC-ARM
| Subscale and Item | Factor Loadings | ||
| 1 | 2 | 3 | |
|
Relational (Eigenvalue = 12.70, 47.05% of variance) |
|||
| 5. My family has usually supported me through life. | .70 | -.14 | -.08 |
| 14. I feel supported by my friends. | .66 | -.10 | .01 |
| 17. My family stands by me during difficult times. | .82 | .00 | -.30 |
| 18. My friends stand by me during difficult times. | .95 | .15 | .02 |
| 21. I know where I can get help in my community. | .60 | -.00 | .12 |
| 24. I feel secure when I am with my family. | .50 | -.03 | .30 |
| 25. I have opportunities to be useful in life (like skills, a job, caring for others). | .54 | -.19 | .18 |
|
Personal (Eigenvalue = 2.04, 7.54% of variance) |
|||
| 1. I cooperate with people around me. | .35 | -.51 | -.17 |
| 2. I have people I can respect. | .36 | -.56 | .11 |
| 3. Getting qualifications or skills is important to me. | .02 | -.80 | -.85 |
| 4. I know how to behave in different social situations. | -.13 | -.83 | .13 |
| 8. I try to finish what I start. | .17 | -.75 | .03 |
| 11. People think that I am fun to be with. | .01 | -.60 | .09 |
| Cultural
(Eigenvalue = 1.77, 6.54% of variance) |
|||
| 6. I am proud of my ethnic background. | -.34 | .26 | .43 |
| 9. Spiritual beliefs are a source of strength for me. | -.27 | -.02 | .48 |
| 10. My family knows a lot about me. | -.17 | -.09 | .64 |
| 12. I talk to my family about how I feel. | .04 | -.12 | .79 |
| 16. I feel I belong to my community. | -.27 | .13 | .51 |
| 20. I have opportunities to show others that I can act responsibly. | -.13 | .26 | .46 |
| 22. I participate in organized religious activities. | .121 | .33 | .54 |
| 26. I enjoy my family’s cultural and family traditions. | .17 | .17 | .87 |
| 27. I enjoy my community’s culture and traditions. | -.04 | .25 | .50 |
Note. These 22 items are rated on a 5-point scale (1= Not at all to 5 = A lot) and compose the Somali RRC-ARM.
As presented in Table 7, the Somali RRC-ARM subscale intercorrelations using non-weighted factor scores were moderate, ranging from .57 (Individual and Cultural) to .67 (Relational and Cultural). Subscale intercorrelations using weighted factor scores were moderate, ranging from .53 (Individual and Cultural) and .63 (Relational and Cultural; Table 8). This justifies the use and interpretation of separate subscales (instead on one overall factor), in that although all subscales reflect the general construct of resilience (as evidenced by the positive intercorrelations), each subscale still seem to uniquely tap specific manifestations of the construct; (at most, any two subscales share only 47.6% of the variance).
Table 6
Somali RRC-ARM Unweighted (Weighted) Subscale Intercorrelations
| Individual | Relational | Cultural | |
| Somali RRC-ARM:
Individual |
1 | – | – |
| Somali RRC-ARM:
Relational |
.62** (.59**) | 1 | – |
| Somali RRC-ARM:
Cultural |
.57** (.53**) | .67** (.63**) | 1 |
*p < .05.
**p < .01, one-tailed test of statistical significance.
Reliability of the Somali RRC-ARM
Non-weighted inter-item correlations among the 22 Somali RRC-ARM items ranged from .04 to .76 with an average correlation coefficient of .43 (moderate correlation). The overall Cronbach’s alpha (non-weighted) was .94. For the non-weighted subscale scores, the Cronbach’s alphas were as follows: Factor 1 (Individual) = .87, Factor 2 (Relational) = .90, and Factor 3 (Cultural) = .89. Weighted inter-item correlations ranged from .04 to .77 with an average correlation coefficient of .43 (moderate correlation). The overall Cronbach’s alpha (weighted) was .93. For the weighted subscale scores, the Cronbach’s alphas were as follows: Factor 1 (Individual) = .86, Factor 2 (Relational) = .89, and Factor 3 (Cultural) = .87. These scores suggest little difference between non-weighted and weighted factor scores. Thus, the following results reflect analyses with non-weighted factor scores only.
Within-Subject Differences on Somali RRC-ARM and MLQ Subscales
A repeated-measures ANOVA was conducted to evaluate whether participants’ Somali RRC-ARM subscale scores (Individual, Relational, Cultural) differed significantly from one another. The results indicated that participants’ subscale scores did not differ significantly from one another, F(1,136) = 2.95, p = .054. A paired-samples t test was conducted to evaluate whether participants’ presence of meaning in life (MLQ-P) scores differed significantly from their search for meaning in life (MLQ-S) scores. The results indicated that participants’ presence of meaning in life (MLQ-P) scores (M = 5.98, SD = 1.29) were significantly higher than their search for meaning in life (MLQ-S) scores (M = 4.57, SD = 1.64), t(133) = 7.72, p < .001.
Relationships Between the Somali RRC-ARM and Other Study Measures
Convergent validity
As presented in Table 7, the Somali RRC-ARM full scale and subscale scores had theoretically consistent and statistically significant positive correlations with the personal well-being (PWI-A), ranging from .42 to .64. Also, the Somali RRC-ARM full scale and subscale scores had theoretically consistent and statistically significant positive correlations with presence of meaning in life (MLQ-P) subscale scores, from .49 to .69. Furthermore, the Somali RRC-ARM full scale and subscale scores also had theoretically-consistent negative correlations with post-migration difficulties in life (PMLD), with all correlations reaching statistical significance except for one (Factor 1: Cultural Resilience). These findings provide support for the convergent validity of the Somali RRC-ARM.
Table 7 Intercorrelations between Somali RRC-ARM and Other Study Measures
| Personal Well-being (PWI-A) | Presence of Meaning (MLQ-P) | Search for Meaning (MLQ-S) | Post-migration Life Difficulties (PMLD) | |
| Somali RRC-ARM:
Overall |
.64** | .69** | .02 | -.29** |
| Somali RRC-ARM: Individual | .42** | .49** | .08 | -.21** |
| Somali RRC-ARM: Relational | .57** | .59** | -.09 | -.42** |
| Somali RRC-ARM:
Cultural |
.63** | .68** | .06 | -.14 |
*p < .05.
**p < .01, one-tailed test of statistical significance
Incremental validity
None of the bivariate correlations between personal well-being (PWI-A) and status variables (i.e., age, length of time living in US, level of education, marital status, and income) were statistically significant, with none of the correlations exceeding .15. Furthermore, search for meaning in life (MLQ-S) was also not significantly correlated with personal well-being (r = -.10, p = .13). However, given that post-migration difficulties (PMLD) and presence of meaning in life (MLQ-P) significantly correlated with personal well-being (PWI-A), we examined whether the Somali RRC-ARM predicts well-being above and beyond the presence or absence of post-migration difficulties and/or presence of meaning in life. See Table 8 to review intercorrelations between study measures.
Table 8 Intercorrelations between Study Measures
| Personal Well-being (PWI-A) | Presence of Meaning
(MLQ-P) |
Search for Meaning
(MLQ-S) |
Post-migration Life Difficulties (PMLD) | |
| Personal Well-being
(PWI-A) |
1 | |||
| Presence of Meaning (MLQ-P) | .78** | 1 | ||
| Search for Meaning (MLQ-S) | -.10 | -.02 | 1 | |
| Post-migration Life Difficulties
(PMLD) |
-.19* | .75** | .27* | 1 |
*p < .05.
**p < .01, one-tailed test of statistical significance
A hierarchical regression analysis was conducted to test the hypothesis that resilience (Somali RRC-ARM) accounts for significant variance in personal well-being (PWI-A) above and beyond the contributions of post-migration difficulties in life (PMLD) and presence of life meaning (MLQ-P) on well-being. The total personal well-being score (PWI-A) was entered as the outcome variable. The predictor variables were entered starting with post-migration difficulties (PMLD) in the first step, then the ‘presence of meaning’ subscale of the MLQ in the second step, and the Somali RRC-ARM in the third and final step.
The results of the hierarchical regression are presented in Table 9, showing that significant R2 statistics were obtained for each predictor. The significant R2 change statistic beginning in the second step suggested higher scores on presence of meaning in life subscale of the MLQ predicted a statistically significant amount of variance in personal well-being (PWI-A) above and beyond that predicted by presence or absence of life difficulties. The significant R2 change statistic present in the third step suggests the Somali RRC-ARM predicted unique variance in personal well-being not accounted for by presence of meaning in life (MLQ-P) and post-migration life difficulties (PMLD), supporting the incremental validity of the Somali RRC-ARM. These results suggest the Somali RRC-ARM predicts unique variance (2.0%) in personal well-being, which is evidence that supports its incremental validity and clinical utility (Hunsley & Meyer, 2003).
Table 9 Summary of Hierarchical Regression Analysis for Variables Predicting Personal Well-being
| Model 1:
Post-migration Life Difficulties (PMLD) |
Model 2:
Post-migration Life Difficulties (PMLD) + Presence of Meaning (MLQ-P) |
Model 3:
Post-migration Life Difficulties (PMLD) + Presence of Meaning (MLQ-P) + Resilience (Somali RRC-ARM) |
|||||||
| Variable | B | SE B | β | B | SE B | β | B | SE B | β |
| PMLD | -.60 | .26 | -.19* | -.16 | .17 | -.05 | -.06 | .18 | -.02
|
| MLQ | 1.33 | .10 | .76** | 1.12 | .13 | .64**
|
|||
| Somali RRC-ARM | .66 | .27 | .19* | ||||||
| R2 | .04
5.10* |
.60
180.87** |
.62
5.92* |
||||||
| F for change in R2 | |||||||||
*p < .05.
**p < .01, one-tailed test of statistical significance
Chapter 6: Integrated Discussion of Study Findings
Theoretically and methodologically aligned with the work of the International Resilience Project (IRP), this study employed a participatory, sequential, mixed-method research design to: a) culturally adapt and validate the RRC-ARM for use with Somali refugees; and b) explore resilience in the context of Somali culture and forced displacement.
An exploratory factor analysis of the RRC-ARM produced a three-factor structure. The overall Somali RRC-ARM and the factor scales (Individual, Relational, and Cultural) demonstrated good internal consistency. The Somali RRC-ARM also demonstrated good convergent validity. The measure positively associated with personal well-being and presence of meaning in life. The Somali RRC-ARM also negatively correlated with life difficulties. This pattern of correlations provides support for the convergent validity of the Somali RRC-ARM. Evidence was also found to support the incremental validity of the measure, in that the Somali RRC-ARM predicted a significant amount of variance in personal well-being (PWI-A), above and beyond that predicted by the absence of post-migration life difficulties (PMLD) and presence of meaning in life (MLQ-Presence). These quantitative findings provide support for the reliability and validity of the 22-item Somali RRC-ARM, the first psychometrically-validated measure of resilience for Somali refugees.
It was also found that resilience (Somali RRC-ARM) was positively associated with presence of meaning in life (MLQ-Presence), and presence of meaning in life predicted a good portion of variance in personal well-being. The qualitative findings suggest “presence of meaning in life” is reflective of the broader cultural influence of Islam on understanding of life experiences in the context of Somali culture. Islam emerged throughout the qualitative data as an influential component of resilience. Abdullahi (2001) suggests that Islamic faith provides a framework from which Somali people understand life experiences. Many studies have shown an association between religion, meaning in life, and well-being (e.g., Park, 2005). These previous findings are consistent with qualitative and quantitative findings in this study that suggest Islam resonates a sort of “existential resilience” among a vast network of Somali people across many countries around the globe. The qualitative results also suggest that resilience resides within broader geographic, political, and cultural contexts. The resilience process involves behavioral navigation of the context toward health-sustaining resources (i.e., food, water, safety, opportunity, health, and subjective sense of well-being), and negotiation for these health-sustaining resources, in culturally meaningful ways (Ungar, 2008). Resilience involves goodness-of-fit between an individual’s navigation strategies with the context in which the strategy is attempted (Ungar, 2008).
In this final chapter, qualitative and quantitative findings are integrated into a proposed Somali Multidimensional and Multilevel Resilience (SMMR) Model. The SMMR Model and each of its components are discussed as related to individual and collective expressions of resilience across contexts. Practical implications of the SMMR Model for refugee resettlement programs, development/delivery of educational and employment resources, and provision of health and behavioral healthcare services are then discussed. Finally, methodological implications for resilience researchers interested in applying mixed-methodology and participatory feedback to culturally-centered and community-focused research locally and globally are presented.
Somali Multidimensional and Multilevel Resilience (SMMR) Model
Integration of qualitative and quantitative findings resulted in the following conceptualization of resilience: resilience in the context of Somali culture and forced displacement is an interactive process between individual, relational, and cultural “systems” that results in successful navigation toward, and negotiation for, culturally-defined and contextually-bound health-sustaining resources. Based on this definition, and in collaboration with Somali cultural advisors, we developed the SMMR Model. The SMMR Model provides a framework from which to qualitatively and quantitatively assess individual, relational, and cultural factors that support navigation toward, and access to, health-sustaining resources and opportunities for personal growth and enhancement across contexts. Humanitarian-aid organizations, refugee-resettlement programs, and healthcare providers may find the model useful for approaching work with Somali refugees from a strengths-based perspective. See Figure 4 to view the proposed, working model of the SMMR. This is followed by a discussion of each component of the model as related to Somali refugee experience.
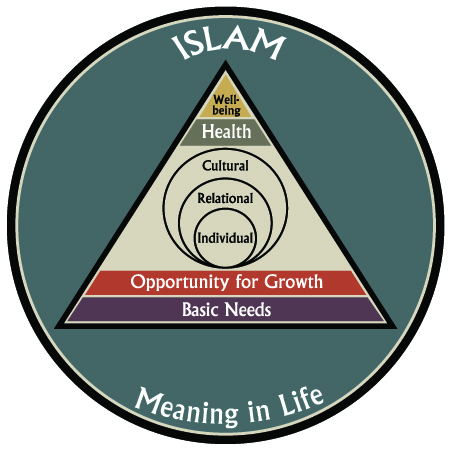
Figure 4. Somali Multidimensional and Multilevel Resilience Model (SMMR)
Consistent with Bronfenbrenner’s (1979) ecological model, the innermost circle of the SMMR Model represents the individual: biological makeup, personality, and individual life experiences. All other levels of the model impact the individual’s development in (and experience of) the world. The individual is embedded in the family system and other relational networks. The individual, his or her family system and other relational networks are embedded in cultural values, beliefs, and behaviors. These three levels of the model (individual, relational, and cultural) are consistent with the quantitative findings of this study; these are the three factors that emerged through EFA of the Somali RRC-ARM. Simply measuring these three levels quantitatively with the Somali RRC-ARM, however, does not capture the more fluid, process-oriented, and interactive aspects of resilience. These aspects of resilience seem more amenable to qualitative methodology.
For example, the quantitative findings revealed a strong, positive association between presence meaning in life, resilience, and well-being. Based on the qualitative findings, however, we interpreted “meaning in life” as an expression of Islamic faith, which most participants identified. Other aspects of life also emerged from the qualitative data that provide a sense of meaning and purpose in life, such as family, children, and the ability to contribute to the broader community. The SMMR Model presents Islam and meaning in life as forms of “existential resilience” that resonate throughout the model promoting personal and collective sense of meaning and purpose, even in the context of marked adversity.
Context
The SMMR Model, as presented above, is intended to be placed within the particular context in which resilience is being examined. Careful consideration of context is important to resilience research as context influences the human experience on all levels (Ungar, 2008). The individual develops in context from the moment of conception. Maternal access to health-sustaining resources, for example, impacts the prenatal environment (e.g., nutrition, avoiding known teratogens) and subsequent health of the infant (Arnett, 2012). Political policies influence safety, security, and distribution of resources throughout the environment, which in turn impact individual development (Daiute, 2012).
During the qualitative phase of this study, resilience was examined across three distinct contexts (i.e., Somalia, refugee camps, and the US). Based on the qualitative findings, emergent contextual factors that influenced resilience (as a process and outcome) among Somali refugees included: geographic location, climate, and weather; historical context and political structure; safety and security in the environment; availability of sustainable resources; and accessibility of health-sustaining resources (e.g., food, water, safety, education, employment). These contextual factors placed boundaries around the experience of resilience.
The climate of Somalia is semi-arid and vulnerable to drought (Abdullahi, 2001). Since the onset of civil war in the country, two severe draughts have contributed to famine and increased violence in the region (Abdullahi, 2001; Putnam & Noor, 1993).
Based on the qualitative findings, health-sustaining resources (i.e., food, water, safety, opportunity for growth, health, and well-being) were severely limited in Somalia due to geographic and climatic considerations, and political violence contributed to disproportionate access to health-sustaining resources. Access to basic health resources became the primary motivator of behavior.
Key-informants described refugee camps as only slightly better than Somalia. The geography and climate of Eastern Kenya (where most of the camps are located) are similar to Somalia (Abdullahi, 2001), contributing to harsh living conditions with less than adequate shelter in the camps. Basic resources were severely limited and lack of safety continued to be a problem. Key-informants described rape and murder as somewhat regular occurrences in refugee camps and behavior was adjusted based on these realities.
Based on these findings, “resilient” Somali refugees are those who develop strategies to gain access to some degree of health-sustaining resources and thereby, engender subjective well-being in the context of adversity. Behavioral strategies that were functional (i.e., “resilient”) in Somalia and in refugee camps, however, may not be functional in the US. For example, key-informants described how young women were typically kept close to their personal camp and not allowed to venture around camp alone, often limiting their access to potential opportunities for growth and development. This was to protect them from the dangerous context in which they were living. Once in the US, it is no longer “functional” to keep a young girl at home for safety. Young women are expected to attend school and gain some degree of independence from their family unit.
Key-informants described better conditions in the US in terms of increased access to basic resources and safety and more opportunities for growth and development. Geography and climate, however, emerged as an important contextual factor in the US with some key-informants discussing difficulty adjusting to cold environments and others describing difficulty adjusting prayer times and annual religious celebrations to the rapidly changing patterns of daylight in Alaska, for example. Other contextual factors that emerged from both qualitative and quantitative findings included exposure to racial discrimination, communication difficulties, and difficulties gaining employment in the US.
The point here is that context places boundaries around access to health-sustaining resources. Context, therefore, shapes behavior into contextually functional patterns that result in increased access to health-sustaining resources. Functional behavior in one context may not be functional in another context (Hayes, Strosahl, & Wilson, 2012). This shift in behavior from context-to-context can present challenges for refugee populations and is essential to understanding resilience in context. Based on this study, if an individual successfully navigates the personal context toward health-sustaining resources, successfully negotiates for those resources, and is able to position his or her behavior within the broader cultural context (most often through an Islamic framework), the behavioral process is likely experienced as resilient.
Health-sustaining resources
In this study, health and health-sustaining resources were examined both qualitatively and quantitatively. Based on the qualitative findings, health-sustaining resources emerged in a hierarchy based on need (Maslow, 1943). At the base of the hierarchy are basic needs. Access to food, water and safety are at the base. Without access to these basic needs, consideration of “higher-order” resources becomes less likely. Once basic-needs are reasonably well-met, opportunity for growth emerged as an important resource in the aim for health and well-being. Opportunities for growth include endeavors that increase access to material resources, as well opportunities that increase subjective sense of meaning in life and personal well-being.
Opportunities for growth vary from context-to-context
In refugee camps, for example, opportunities for growth that emerged from the qualitative data were comprised of labor-oriented work in the camp (e.g., digging latrines, constructing infrastructure) or migration away from the camp for opportunities elsewhere (often to Nairobi). According to key-informants, this work was poorly paid, if paid at all. But many of the key-informants described seeking work opportunities nevertheless because they provided some structure to the day and contributed to a sense of purpose in life.
Opportunities for growth that emerged from the qualitative data in the context of Somalia and in the US were more education- and employment- (or business-) oriented. Education emerged from the qualitative data as a culturally valued resource across contexts. The form education assumed, however, was somewhat defined by the context in which the education was being delivered. One key-informant, who grew up as a nomadic herder in Somalia, described his education in this context. Structured by age and divided by gender, children are mentored into their role in the community. More formal systems of education emerged from the qualitative data in the US and in urban areas of Somalia, where educational opportunities take a form more consistent with a Western model of education. Higher education is highly valued and many Somali people live very successful, business-oriented lifestyles (Abdullahi, 2001).
Based on the qualitative data, opportunities for growth across contexts involve gradual assumption of responsibility among the family system and increased ability to contribute to collective well-being. Ability to contribute to the greater community emerged from the qualitative data as an important aspect of well-being, and loops back around to living a collaborative, Islamic lifestyle. Contribution emerged as an important element that provides a sense of meaning and purpose to life. While opportunities for growth typically include increased access to material resources (e.g., food, water, healthcare, money), it is also important to consider how these opportunities for growth also increase one’s ability to structure their life in the context of adversity and find meaning and a sense of purpose in life following what is often a series of traumatic events.
Some key-informants mentioned absence of physical and mental illness as indicators of health, but emergent themes in the qualitative data brought attention to the important role of spiritual health and well-being. Spiritual well-being was described as the pinnacle from which all other expressions of health emerge (e.g., “Health all goes under spirituality.”). This concept is captured at the top level of pyramid—the peak is labeled well-being.
Individual, relational, and cultural factors
Based on the qualitative results, the “resilient” Somali individual was described as determined, future-oriented, goal-directed, and assertive. The quantitative findings suggest individual-level items that clustered together on the Somali RRC-ARM included those that involved cooperation with others, social/behavioral intelligence, goal-orientation, and interpersonal savvy. See Figure 5 to review Somali RRC-ARM items that loaded at the individual-level.
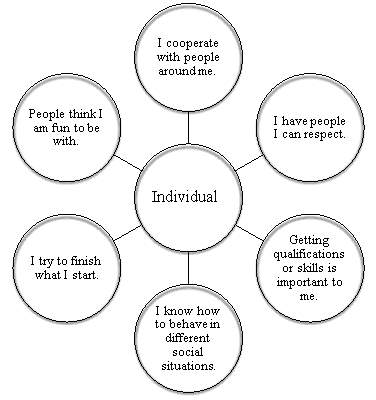
Figure 5. Somali RRC-ARM Individual Factors of Resilience
Interpretation of individual-level factors of resilience, however, cannot be considered outside of the family/relational context. Based on qualitative findings, relational networks propel individual resilience factors into motion through opportunities for personal and collective growth, physical and emotional health, and subjective sense of well-being. Consistent with the qualitative findings, relational-level items that clustered together on the Somali RRC-ARM included those that captured emotional and social support, sense of security within the family, knowledge of supportive networks in the community, and opportunities to contribute to the broader community. See Figure 5 to review Somali RRC-ARM items that loaded at the relational-level.
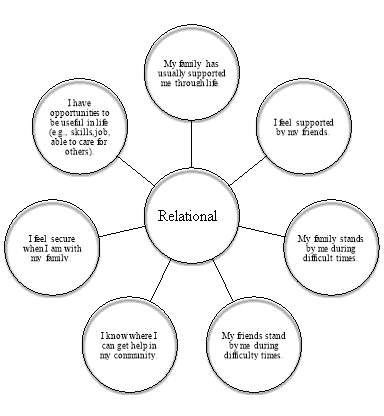
Figure 6. Somali RRC-ARM Relational Factors of Resilience
Consistent with past literature (Abdullahi, 2001; Putnam & Noor, 1993), key-informants used the term “family” beyond the Western view of a nuclear family and included aunts, uncles, cousins, and neighbors. Children were described as highly valued by Somali culture. They provided a source of hope for the future and a conduit for transmission of religious and cultural values and traditions. Nurturing Islamic values in children is of primary importance (Abdullahi, 2001). The Somali family system serves as a conduit of social and emotional support across contexts. Moreover, family and relational networks promote collective resource sharing and mobility across contexts.
Somali key-informants described the notion of family as inseparable from culture. Collective needs of family relations are placed before individual needs, and decisions are made within the family structure. The qualitative findings suggest that cultural factors of resilience among Somali refugees include affiliation with a religious organization, having a life philosophy, and cultural and/or spiritual identification (e.g., feeling culturally grounded by knowing where one comes from and being part of a cultural tradition that is expressed through daily activities). Consistent with the qualitative results, the quantitative findings revealed that cultural-level items that clustered together on the Somali RRC-ARM included items related to ethnic pride, spiritual beliefs, family openness and communication, sense of belonging, purpose in life, and ability to contribute to the family system. See Figure 7 to review Somali RRC-ARM items that loaded at the cultural-level.
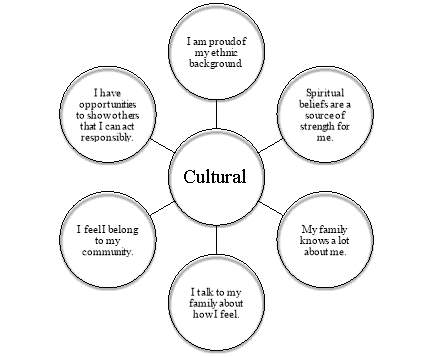
Figure 7. Somali RRC-ARM Cultural Factors of Resilience
Consistent with other research with Somali people, nearly all participants in this study identified as Muslim (e.g., Bentley, 2011). Based on the qualitative findings, Islam seems to provide an explanatory model for making sense of life experiences and contributes to presence of meaning and purpose in life. Based on quantitative findings, presence of meaning and purpose in life is an important predictor of well-being. The qualitative findings suggest health and well-being is defined through the context of Islamic spiritual beliefs. That is, freedom from physical and mental illness, the ability to contribute to the family system and broader community, all depend on God’s Will and one’s commitment to spiritual faith and practice of an Islamic way of life.
Islam and meaning in life
Based on both qualitative and quantitative findings, a “field” of existential resilience was included around the entire model. This is to demonstrate what is thought to be a culturally-specific and very strong contributor to resilience in the context of Somali culture. Islamic faith seems to contribute to well-being across contexts. This component of the model is based on the qualitative findings indicating that Islam and meaning in life are important and intertwined concepts among Somalis across contexts. The quantitative results showing that resilience and meaning in life are important contributors to personal well-being are also consistent with this feature of the SMMR Model.
Many studies have shown a positive relationship between religion and presence of meaning in life, and that both are related to positive coping when faced with significant adversity (summarized by Park, 2005). For example, Pan, Wong, Chan, and Joubert (2008) identified religion and presence of meaning in life as protective factors among international students when adjusting to foreign environments. Search for meaning in life is less consistently documented as a helpful component of coping. Specifically, searching for meaning in life and not finding the meaning may actually relate to decreased well-being (Baumeister, 1991; Steger et al., 2006; Steger, Kashdan, Sullivan, & Lorentz, 2008). Consistent with this previous research, the quantitative findings in this study showed participant scores on presence of meaning and search for meaning differed significantly; presence of meaning in life positively associated with resilience and well-being while search for meaning in life failed to produce a significant relationship with those constructs.
Now that the qualitative and quantitative findings have been discussed in terms of how they informed the creation of the SMMR Model, and that each component of the SMMR Model has been described, I now turn toward some example scenarios wherein the SMMR Model may be applied at the individual, community/organizational, and national levels.
Example One: Applying the SSMR Model at the Individual Level
“Aden” is a 34-year-old man who lives with a large family in a US city. He has nine children of his own. He resettled in the US almost 10 years ago. Aden was forcibly displaced from his home when he was 14. He successfully navigated his way through refugee camps eventually resettling in the US. According to Aden, he lives well in the US. He has a large family, a good job, and a strong network of family relationships across the US. and elsewhere. A member of the Somali community identifies Aden as an example of resilience in the context of Somali culture and forced displacement. Aden opened his interview by sharing this story:
I left Somalia in 1991, age 14. That is something I remember exactly. There were rebels killing everybody. My dad died when the civil war break out. There was no choice but to leave the country. Thankfully I left with my mom, my sisters, and brothers. Many weeks we travel through the bush. You can’t go by road because there was gunfire and you don’t know who is who because there were so many rebels. We going through the bush for 21 days… no food… no water. It was hot, the summer season we call Jeelel. The dust in your face, you’re thirsty. You cannot get water. No shelter. We came to Kenya refugee camp on the border of Somalia and Kenya. There was over 400 or 500,000 people there, all fleeing Somalia.
Aden’s mother went back to Somalia at one point to gather belongings from their home and never returned. She was killed during the journey home. Aden and his younger brothers lived between a refugee camp in Kenya and an apartment in Nairobi. Aden worked, as did his younger siblings, as they got older. Eventually, Aden married a woman who helped the family system with cooking and caretaking. They began having children.
They applied for resettlement early on but it took ten years before they were resettled in the US. Once resettled, Aden focused on employment. He was bilingual and was able to interpret for the Somali community. At one point he sought higher education but met barriers based on his refugee status and lack of documentation of education. His children attend public schools and his wife takes care of the children and domestic responsibilities while Aden works and earns financial income to support family needs. Using the SMMR Model on the presented information, an individual-level assessment of Adens’s resources is below:
Individual resilience factors:
- Determination
- Self-efficacy
- Forward-focus, action-orientation
Relational resilience factors:
- Large family system
- Marriage and reproduction
- Social and emotional support
- Resource sharing
- Supports migration from location-to-location
Cultural resilience factors:
- Strong Iman
- Sense of meaning and purpose in life
- Contribution to family and community
Contextual resilience factors:
- Geographic location
- Availability of sustainable resources
- Accessibility of sustainable resources
- Political structures and social structure that support access to health-sustaining resources
Example Two: Applying the SSMR Model at the Community Level
Considering resilience from the perspective of capacity building and collective expressions of the construct, The Worldwide Somali Students and Professional (WSSP) Network provides an excellent example of resilience. WSSP is a grassroots, non-profit, community organization of Somali people across the globe committed to delivering on the needs of Somali people living in Somalia and restoring peace to their homeland. This organization is committed to apolitical, solution-focused movement in Somalia, aimed at moving forward in a unified way and reclaiming their homeland. WSSP has excellent representation on the Internet and social media sites. The website includes a description of WSSP mission statement, current activities, and documentation of past activities.
Operation Restore Home 2012
WSSP recently sent a group of students and professional to Somalia in an effort called Operation Restore Home. Their focus was on agriculture, healthcare, and education. Video documentation of Operation Restore Home 2012 is available at this website: http://worldwidesomalistudents.com/media. The WSSP organization is demonstrative of a community organization functioning from a resilience perspective. The group has organized around a shared vision and action-orientation. The following excerpt is from their website:
The Worldwide Somali Students and Professionals (WSSP) is a global movement that exists to mobilize young Somalis to use their talents, work together and address the unmet needs of a proud people. WSSP is a nonprofit, non-political movement. We are young, modern and believe in doing good for the sake of our people rather than our clan or familial affiliations. Our members are the engineers, doctors, nurses, teachers, Earth scientists and future leaders of our people. They are from Somalia, Kenya, Ethiopia, Djibouti, and Somalia and are scattered across all the major continents of the world (directly quoted from the website http://worldwidesomalistudents.com/).
Using the SMMR Model on the presented information, a community-level assessment of the WSSP Network is below:
Individual resilience factors:
- Collaboration
- Future-orientation
- Solution-focused
Relational resilience factors:
- Resource sharing
- Collective self-efficacy
Cultural resilience factors:
- Somali ethnic, national pride
- Culturally grounded, indigenous strategies for solution
- Tolerance for different ideologies and beliefs
Contextual resilience factors:
- Access to technology and use of social media (e.g., Facebook, Twitter) has increased collaborative power of WSSP.
Example Three: Applying the SMMR Model at the National Level
Consider the problem of piracy along the coastline of Somalia. Government and public opinion largely considers piracy behavior delinquent, harmful, and dysfunctional. A contextual analysis of piracy behavior, however, presents the behavior as a very effective way of accessing health-sustaining resources in the context of sustained adversity. Somali “pirates” have developed from the time of conception in Somalia. They have survived two famines and over 20 years of civil war. Limited access to health-sustaining resources (water, food, safety, and security) is the norm, not the exception in their life.
This “delinquent, harmful, and dysfunctional behavior” of piracy may actually be an expression of resilience in the context of Somalia. An individual faced with death or survival may choose survival by joining a group that allows access to health-sustaining resources (food, water, safety, opportunity) and provides a sense of structure, meaning and purpose in life that has otherwise been devastated.
The point here is not to defend piracy behavior involvement as practical solutions for the challenges faced in Somalia, but to demonstrate how resilience, as a psychological construct and behavioral process, takes form in culturally and contextually functional ways. Human behavior occurs in context. Context determines the functionality of behavior. Exploring behavior in context can shed light on the functionality of particular patterns of behavior in context (Hayes et al., 2012). The interaction between the individual and context leads to particular behavior patterns that may or may not contribute to resilience depending on the culture and context in which the behavior occurs. Using the SMMR Model on the presented information, an assessment of Somali piracy is below:
Individual resilience factors:
- Collaboration
- Future-orientation
- Solution-focused
Relational resilience factors:
- Resource sharing
- Collective self-efficacy
Cultural resilience factors:
- Somali ethnic, national pride
- Culturally grounded, indigenous strategies for solution
Contextual resilience factors:
- Limited resources
- War and violence
Implications
In addition to facilitating a better and more complex understanding of the construct of resilience as conceptualized and experienced by Somalis, the SMMR Model also provides a framework to evaluate and improve provision of resources across contexts in culturally responsive and contextually realistic ways. The SMMR Model can inform practice across a number disciplines. Discussed here are: (1) refugee resettlement practices in the US; (2) medical and behavioral healthcare provision in the US; (3) next steps in research on resilience in the context of Somali culture and forced displacement; and (4) applications of the Somali RRC-ARM and SMMR Model to program development, evaluation, and clinical practice.
Refugee resettlement and post-migration adaptation
Many refugees struggle post-migration with difficulties related to adjustment to life in the US (Porter & Haslam, 2005). High rates of medical and mental health problems are documented among Somali refugees (Bhui et al., 2003; Halcón et al., 2004; Jaranson et al., 2004; Roodenrijs et al., 1998). Greater access to education and employment supports positive post-migration adaptation (Bhui et al., 2006). These findings are consistent with this study. Education and employment are culturally-valued, health-sustaining resources that emerged in our examination.
Refugee resettlement in the US typically includes programs that support new refugees, including case management for each individual and/or family, educational opportunities (e.g., English language classes, public education for youth), and employment support services (Office of Refugee Resettlement, 2013). These resources seem to be important facilitators of post-migration resilience (Bhui et al., 2006). Government and local funding sources support refugee resettlement programming. Continued funding of refugee resettlement programming, as well as thoughtful utilization of these resources, is important to successful refugee resettlement policy and practice in the US.
Refugee resettlement programs could utilize the SMMR Model to assess individual refugees (or new groups of refugees) for resilience factors across all levels of the model. Administration of the Somali RRC-ARM would provide a brief, quantitative evaluation of individual, relational, and cultural factors. An interview or group discussion could contribute information about health-sustaining resources and the processes by which these resources are navigated and negotiated. Resettlement planning and programming could build on inherent strengths of the individual or group and work to facilitate access to identified health-sustaining resources.
Educational and employment programming
It is recommended that educational programming be delivered in contextually responsive and culturally meaningful ways. For example, before considering educational and employment programming, first assess for access to basic resources (e.g., food, water, safety, security). Focus on meeting these needs first. Create positive social and culturally responsive learning environments aimed at teaching the English language and supporting the process of integration into the US context.
Educational programming could include:
- Provision of on-site childcare by Somali community members during all classes;
- Cultural and community orientation offered by members of Somali community and members of local community;
- Access to quality English Language education program;
- Community education and advocacy for inclusive work and social environments, mutual learning, and respect for cultural beliefs and values in practice.
It is recommended that employment programming consider social structure, childcare provision, integration of cultural practices into daily life, and contextual boundaries to successful employment experiences. The degree to which the local community is accustomed to working alongside diverse peoples will influence the new refugee experience. In large communities, like Minneapolis, employers and community members are accustomed to Somali cultural practices and adapt to support religious practices during the workday. In smaller communities, like Anchorage, employers and community members are far less accustomed to Somali cultural practices and may be less likely to adapt and support religious practices during the day. Public education and community advocacy may be necessary in a community that is new to resettled refugees to help support the process.
The SMMR Model could be used to develop culturally and contextually realistic educational and employment programming. Administration of the Somali RRC-ARM along with gathering qualitative information about the culture and context in which education and employment is sought can inform the development and provision of these resources in useful ways.
Medical and behavioral healthcare service provision
Healthcare providers and community programs working with Somali people could gain much from adopting a resilience perspective through which to conduct medical health, mental health, and social service assessments. Somali people may be more open to sharing about resilience and resources based on their level of need in context. This openness can contribute to healthful relationship development between clinician/caseworker and client. Administration of the Somali RRC-ARM and a brief conversation about various domains of resilience as outlined by the SMMR Model could contribute to development of individualized health interventions or community programming congruent with individual values in the context of the broader refugee experience.
Interaction with the medical community can be a challenging experience for many individuals who do not speak English. The use of medical interpreters is essential to provision of appropriate health care and even required by law if an organization accepts federal funding for operations (e.g., Medicaid). Research is needed to improve understanding of communication through interpreters. What are the needs of patients/clients when receiving medical information from healthcare providers? What are the needs of healthcare providers when providing healthcare information to patients/clients? What are the needs of the interpreter who is facilitating the communication between healthcare provider and patient/client? How can we best facilitate transmission of information between healthcare providers and newly resettled populations? But for now, provision of interpreter services is a necessary function of any clinic serving individuals who do not speak English as their first language.
Research methodology
This study extends the work of the IRP by adding to the broader body of literature on resilience among non-Western populations. This was the first study that applied mixed-methodology to the study of resilience among Somali refugees and the first to gather data using the RRC-ARM. The presented findings support the reliability and validity of the RRC-ARM as a measure of resilience among Somali refugees and add to understanding of meaning of life in the context of stress and adversity.
It is strongly recommended to use mixed-methodology and cultural advisors, however, when using the measure. Qualitative data contextualizes quantitative findings and cultural advisors help facilitate culturally responsive direction in research. Future research should include validation of the Somali RRC-ARM among a large sample of Somali people through confirmatory factor analysis. Replication of this research methodology among various refugee populations could add breadth and depth to our understanding of resilience in the context of diverse cultures and forced displacement.
Program evaluation
International and national organizations and professional groups who work with Somali people may find the SMMR Model helpful when evaluating programming aimed at promoting positive post-migration adaptation. Administering the Somali RRC-ARM to all refugees who resettled in a particular region in the past year, for example, and conducting a series of interviews with these individuals and other stakeholders in the community, may produce data useful in evaluation of services and improvement of service delivery.
Clinical applications
When working with a Somali individual on a medical or mental- health concern, a resilience approach may allow for exploration of resources and disclosure of important experiences in a culturally respectful way. Integrating family into the clinical process may be helpful if the individual has a strong relational network.
The SMMR Model provides a framework from which one could assess mental health. For example, a clinical interview could: a) gather information about the individual (perhaps some assessment of personality, developmental history, interpersonal style, and unique individual life experience); b) explore family dynamics and relational networks; c) consider cultural beliefs and values and assess for individual adherence to and identification with the culture; and d) place clinical conceptualization and treatment plan in context (e.g., geographic, political).
Limitations
Although this study contributes to a more complete understanding of resilience in the context of Somali culture and forced displacement, it is not without limitations. Results and implications of this study should be considered in the context of these methodological limitations.
In terms of qualitative data collection, we used a snowball sampling strategy. Snowball sampling is often employed when populations are challenging to access. Because participants are not selected from a sampling frame, the snowball sampling is subject to a number of biases that may limit the generalizability of the findings of the study. However, in this study, the snowball sampling strategy was employed in such a way to maximize Somali perspectives on resilience; thus, it is possible that the snowball sampling strategy may have actually increased the trustworthiness of the data.
Also, qualitative data collection was limited to English speaking participants. Language is an essential conduit of emotion and culture. While this is an important limitation, the choice to include only English-speaking participants was based on limited resources for interpretation and the potential errors that may occur during interpretation and transcription of interpreted data. Future research could address this limitation by gathering data in the Somali language.
There are also some limitations on the measures used in the study. While significant effort was made to select culturally relevant measures of variables that may be related with resilience, the MLQ and PWI-A were both developed from Western populations and imposed a Western worldview on the understanding of meaning of life and psychological well-being. This limitation speaks to the need for development of indigenous psychological measures and the need for mixed-methodology in the research of resilience across cultures. Finally, quantitative data collection was facilitated through online media and community organizations in Minnesota and Alaska, limiting the generalizability of findings. Due to the systemic nature of this investigation, it is important to acknowledge that systems vary from context-to-context. Therefore, these findings may not generalize to participants living in other states and certainly the results may not generalize to Somali people living in Somalia or other countries around the work. Future research should address this issue by examining resilience among Somali people on a broader, more comprehensive scale.
Conclusion
Despite these limitations, this study contributes to the literature in a number of ways. This study produced the most comprehensive and complete understanding of resilience among Somali refugees to date. The robust research-design contributes to breadth and depth of understanding of resilience in the context of Somali culture and forced displacement. Collaboration with Somali cultural advisors helped ensure the cultural relevance of the research design, methodology, study measures, and interpretation of study findings. The study produced the first psychometrically validated measure of resilience for use with Somali people (Somali RRC-ARM) and the most comprehensive conceptualization of Somali resilience to date (i.e., the SMMR Model). The findings have practical and scholarly implications regarding practice and research on health and well-being with non-Western populations living around the globe. Future research could expand this work to include Somali people living in different contexts around the world to increase understanding of cross-contextual similarities and differences in expressions of resilience.
References
Abdullahi, M. D. (2001). Culture and customs of Somalia. Westport, CT: Greenwood Press.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders(4th ed.).Washington, DC: Author.
Anthony, E., & Cohler, B. J. (1987). The Invulnerable Child. New York, NY: Guilford Press.
Apfel, R. J., & Simon, B. (2000). Mitigating discontents with children in war: An ongoing psychoanalytic inquiry. In A. C. G. M. Robben, M. M. Suárez-Orozco (Eds.), Cultures under siege: Collective violence and trauma (pp. 102-130). New York, NY US: Cambridge University Press.
Arnett, J. A. (2012). Human development: A cultural approach. Upper Saddle River, NJ: Pearson Education, Inc.
Aron, A., & Aron, E. N. (2003). Statistics for psychology (3rd ed.). Upper Saddle River, NJ: Prentice Hall/Pearson Education.
Bartone, R. T., Ursano, R. J., Wright, K. M., & Ingraham, L. H. (1989). The impact of a military air disaster on the health of assistance workers: A prospective study. Journal of Nervous and Mental Disorders, 177, 317-328. doi:10.1097/00005053- 198906000-00001
Baumeister, R. F. (1991). Meanings of life. New York, NY: Guilford.
Bentley, J. A. (2011). Cross-cultural assessment of psychological symptoms among Somali refugees. Dissertation Abstracts International: Section A or B: Title of Section, 71(issue), 111.
Bentley, J. A., & Olson C. W. (2008). Somali Refugee Mental Health Cultural Profile. Ethno Med. Retrieved from Author http://ethnomed.org/clinical/mental-health/somali-refugee-mentalhealthculturalprofile/?searchterm=Somali%20Refugee%20Mental%20Health%20Cultural%20Profile
Bhugra, D. (2004). Migration, distress and cultural identity. British Medical Bulletin, 69, 129-141. doi:10.1093/mb/ldh007
Bhui, K., Abdi, A., Abdi, M., Pereira, S., Dualeh, M., Robertson, D., … Ismail, H. (2003). Traumatic events, migration characteristics and psychiatric symptoms among Somali refugees: Preliminary communication. Social Psychiatry & Psychiatric Epidemiology, 38, 35-43. doi:10.1007/00127-003-0569-5
Bhui, K., Craig, T., Mohamud, S., Warfa, N., Stansfeld, S. A., Thornicroft, G., … McCrone, P. (2006). Mental disorders among Somali refugees: Developing culturally appropriate measures and assessing socio-cultural risk factors. Social Psychiatry and Psychiatric Epidemiology, 41, 400-408. doi:10.1007/s00127-006-0043-5
Block, J., & Kremen, A. M. (1996). IQ and ego-resiliency: Conceptual and empirical connections and separateness. Journal of Personality and Social Psychology, 70, 349-361. doi:10.1037/0022-3514.70.2.349
Brislin, R. W. (1970). Back-translation for cross-cultural research. Journal of Cross-Cultural Psychology, 1, 185-216. doi:10.1177/135910457000100301
Bromley, E., Johnson, J. G. & Cohen, P. (2006). Personality strengths in adolescence and decreased risk of developing mental health problems in early adulthood. Comprehensive Psychiatry, 47, 315-324. doi:10.1016/j.comppsych.2005.11.003
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bryant, F. B., & Yarnold, P. R. (2000). Principal-components analysis and exploratory and confirmatory factor analysis. In L. G. Grimm, P. R. Yarnold, L. G. Grimm, P. R. Yarnold (Eds.), Reading and understanding multivariate statistics (pp. 99-136). Washington, DC: American Psychological Association.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159. doi:10.1037/0033-2902.112.1.155
Connor, K. M., Davidson, J. R. T., Lee, L. C. (2003). Spirituality, resilience, and anger in survivors of violent trauma: A community survey. Journal of Traumatic Stress, 16, 487-494. doi:10.1023/A:1025762512279
Cummins, R. A., Eckersley, R., Pallant, J., van Vugt, J., & Misajon, R. (2003). Developing a national index of subjective well-being: The Australian Unity Well-being Index. Social Indicators Research, 64, 159-190. doi:10.1023/A:1024704320683
Daiute, C. (2012). Human development & political violence. New York, NY.: Cambridge University Press.
Denzin, N. K., & Lincoln, Y. S. (2008). Strategies of qualitative inquiry (3rd ed.). Thousand Oaks, CA: Sage.
Donnon, T., & Hammond, W. (2007). A psychometric assessment of the self-reported youth resiliency assessing developmental strengths questionnaire. Psychological Reports, 100, 963-978. doi:10.2466/pr0.100.3.963-978
Donnon, T., Hammond, W., & Charles, G. (2003). Youth resiliency: Assessing students’ capacity for success at school. Teaching and Learning, 1(3), 23-28.
El Sarraj, E., Punamäki, R.-L., Salmi, S., & Summerfield, D. (1996). Experiences of torture and ill-treatment and posttraumatic stress disorder symptoms among Palestinian political prisoners. Journal of Traumatic Stress, 9(3), 595-606.
Felsman, K. (1989). Risk and resiliency in childhood: The lives of street children. In T. Dugan & R. Coles (Eds.), The child in our times: Studies in the development of resiliency (pp.56-80). New York, NY: Brunner/Mazel.
Fleiss, J. L., Levin, B. A., & Paik, M. C. (2003). Statistical methods for rates and proportions (3rd ed.). Hoboken, N.J.: J. Wiley.
Friborg, O., Barlaug, D., Martinussen, M., Rosenvinge, J. H., & Hjemdal, O. (2005). Resilience in relation to personality and intelligence. International Journal of Methods in Psychiatric Research, 14, 29-42. doi:10.1002/mpr.15
Friborg, O., Hjemdal, O., Rosenvinge, J. H., & Martinussen, M. (2003). A new rating scale for adult resilience: What are the central protective resources behind healthy adjustment? International Journal of Methods in Psychiatric Research, 12, 65-76. doi:10.1002/mpr.143
Fox, S., & Tang, S. (2000). The Sierra Leonean refugee experience: Traumatic events and psychiatric sequelae. Journal of Nervous and Mental Disease, 188, 490-495. doi:10.1097/00005053_2000080000-00003
Garmezy, N., & Devine, V. (1984). Project competence: The Minnesota studies of children vulnerable to psychopathology. In N. F. Watt, E. J. Anthony, L. C. Wynne, & J. E. Rolf (Eds.), Children at risk for schizophrenia: A longitudinal perspective (pp. 289-303). Cambridge, UK: Cambridge University Press.
Garmezy, N., Masten, A. S., & Tellegen, A. (1984). The study of stress and competence in children: A building block for developmental psychopathology. Child Development, 55, 97-111. doi:10.1111/j.1467-8624.1984.t600276.x
Gerritsen, A. A. M., Bramsen, I., Devillé, W., van Willigen, L. H. M., Hovens, J., & van der Ploeg, H. (2006). Physical and mental health of Afghan, Iranian and Somali asylum seekers and refugees living in the Netherlands. Social Psychiatry & Psychiatric Epidemiology, 41, 18-26. doi:10.1007/s00127-005-0003-5
Halcón, L., Robertson, C. L., Savik, K., Johnson, D. R., Spring, M. A., Butcher, J., … Jaranson, J. M. (2004). Trauma and coping in Somali and Oromo refugee youth. Journal of Adolescent Health, 35, 17-25. doi:10.1016/S1054-139X(03)00328-8
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2012). Acceptance and commitment therapy: The process and practice of mindful change (2nd ed.). New York, NY: Guilford Press.
Hjemdal, O., Friborg, O., Stiles, T. C., Martinussen, M., & Rosenvinge, J. H. (2006). A new scale for adolescent resilience: Grasping the central protective resources behind healthy development. Measurement & Evaluation in Counseling & Development, 39(2), 84-96.
Hunsley, J., & Meyer, G. J. (2003). The incremental validity of psychological testing and assessment: Conceptual, methodological, and statistical issues. Psychological Assessment, 15, 446-455. doi:10.1037/1040-3590.15.4.446
Hurtes, K. P., & Allen, L. R. (2001). Measuring resiliency in youth: The resiliency attitudes and skills profile. Therapeutic Recreation Journal, 35(4), 333-347.
Ingleby, D. (Ed.). (2005). Forced migration and mental health: Rethinking the care of refugees and displaced persons. New York, NY: Springer Publishing Co.
Jaranson, J., Butcher, J., Halcon, L., Johnson, D., Robertson, C., Savik, K., … Westermeyer, J. (2004). Somali and Oromo refugees: Correlates of torture and trauma history. American Journal of Public Health, 94, 591-598. doi:10.2105/AJPH.94.4.591
Kim, G., Torbay, R., & Lawry, L. (2007). Basic health, women’s health, and mental health among internally displaced persons in Nyala Province, South Darfur, Sudan. American Journal of Public Health, 97, 353-361. doi:10.2105/AJPH.2005.073635
Kinzie, J., Sack, W., Angell, R., Clarke, G., & Rath, B. (1989). A three-year follow-up of Cambodian young people traumatized as children. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 501-504. doi:10.1097-00004583-19890700000006
Kleinman, A. (1988). Rethinking psychiatry: From cultural category to personal experience. New York, NY: Free Press.
Klevens, J., & Roca, J. (1999). Nonviolent youth in a violent society: Resilience and vulnerability in the country of Colombia. Violence & Victims, 14(3), 311-322.
Klohnen, E. C. (1996). Conceptual analysis and measurement of the construct of ego-resiliency. Journal of Personality and Social Psychology, 70, 1067-1079. doi:10.1037/0022-3514.70.5.1067
Kobasa, S. C. (1979). Stressful life events, personality, and health: An inquiry into hardiness. Journal of Personality and Social Psychology, 37, 1-11. doi:10.1037/0022-3514.37.1.1
Koltko-Rivera, M. E. (2006). Rediscovering the later version of Maslow’s hierarchy of needs: Self-transcendence and opportunities for theory, research, and unification. Review of General Psychology, 10, 302-317. doi:10.1037/1089-2680.10.4.302
Koshen, H. A. (2007). Strengths in Somali families. Marriage & Family Review, 41, 71-99. doi:10.1300/J002v41n01_05
Kroll, J., Yusuf, A., & Fujiwara, K. (2011). Psychoses, PTSD, and depression in Somali refugees in Minnesota. Social Psychiatry & Psychiatric Epidemiology, 46, 481-493. doi:10.1007/s00127-010-0216-0
Lau, A. D., Cummins, R. A., & McPherson, W. (2005). An Investigation into the cross-cultural Equivalence of the Personal Well-being Index. Social Indicators Research, 72(3), 403-430.
Leech, N. L., & Onwuegbuzie, A. J. (2009). A typology of mixed methods research designs. Quality & Quantity: International Journal of Methodology, 43, 265-275. doi:10.1007/s11135-007-9105-3
Leibenberg, L., & Ungar, M. (Eds.). (2009). Researching resilience. Toronto, ON: University of Toronto Press, Inc.
Liebenberg, L., Ungar, M., and Van de Vijver, F. R. R. (2012). Validation of the Child and Youth Resilience Measure-28 among Canadian youth with complex needs. Research on Social Work Practice, 2, 219-226. doi:10.1177/1049731511428619
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543-562. doi:10.1111/1467-8624.00164
MacQueen, K. M., McLellan, E., Kay, K., & Milstein, B. (1998). Codebook development for team-based qualitative analysis. Cultural Anthropology Methods, 10(2), 31-36.
Maslow, A. H. (1943). A theory of human motivation. Psychological Review, 50, 370-396. doi:10.1037/h0054346
McSharry, S., & Kinney, R. (1992). Prevalence of psychiatric disorders in Cambodian refugees: A community random sample. Unpublished manuscript, Social Research Institute, Graduate School of Social Work, University of Michigan, Ann Arbor, MI.
Médicins Sans Frontières. (2009). Dadaab: The unacceptable price of asylum. Retrieved from Author http://www.doctorswithoutborders.org/publications/article.cfm?id=3622&cat=special-report
Michultka, D., Blanchard, E. B., & Kalous, T. (1998). Responses to civilian war experiences: Predictors of psychological functioning and coping. Journal of Traumatic Stress, 11(3), 571-577.
Mire, S. (2007). Preserving knowledge, not objects: A Somali perspective for heritage management and archaeological research. African Archaeological Review, 24, 49-71. doi:10.1007/s10437-007-9016-7
Mollica, R. F., Donelan, K., Tor, S., Lavelle, J., Elias, C., Frankel, M., & Blendon, R. J. (1993). The effect of trauma and confinement on functional health and mental health status of Cambodians living in Thailand-Cambodia border camps. The Journal of the American Medical Association, 270(5), 581-586.
Mollica, R. F., Wyshak, G. G., Lavelle, J. J., Mollica, R. F., Cui, X. X., Mcinnes, K. K., & Massagli, M. P. (2002). Harvard Trauma Questionnaire. Journal of Nervous and Mental Disease, 190, 158-166.
Momartin, S., Steel, Z., Coello, M., Aroche, J., Silove, D., & Brooks, R. (2006). A comparison of the mental health of refugees with temporary versus permanent protection visas. The Medical Journal of Australia, 185(7), 357-361.
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52(2), 250-260.
Nuechterlein, K. H., Phipps-Yonas, S., Driscoll, R., & Garmezy, N. (1990). Vulnerability factors in children at risk: Anomalies in attentional functioning and social behavior. In J. Rolf, A. S. Masten, D. Cicchetti, K. H. Nuechterlein, & S. Weintraub (Eds.), Risk and protective factors in the development of psychopathology (pp. 445-479). Cambridge, UK: Cambridge University Press.
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). New York, NY: McGraw-Hill.
Office of Refugee Resettlement (2013). Retrieved March 1, 2013 from http://www.acf.hhs.gov/programs/orr
Onwuegbuzie, A., & Leech, N. L. (2005). On becoming a pragmatic researcher: The importance of combining quantitative and qualitative research methodologies. International Journal of Social Research Methodology, 8, 375-387. doi:10.1080/13645570500402447
Oshio, A., Kaneko, H., Nagamine, S., & Motoyuki, N. (2003). Construct validity of the Adolescent Resilience Scale. Psychological Reports, 93, 1217-1222. doi:10.2466/pr0.2003.93.3f.1217
Paardekooper, B. B., de Jong, J. T. V. M., & Hermanns, J. M. A. (1999). The psychological impact of war and the refugee situation on South Sudanese children in refugee camps in Northern Uganda: An exploratory study. The Journal of Child Psychology and Psychiatry and Allied Disciplines, 40(4), 529-536.
Palmer, D. (2006). Imperfect prescription: Mental health perceptions, experiences and challenges faced by the Somali community in the London Borough of Camden and service responses to them. Primary Care Mental Health, 4(1), 45-56.
Pan, J.-Y., Wong, D. F. K., Chan, C. L. W., & Joubert, L. (2008). Meaning of life as a protective factor of positive affect in acculturation: A resilience framework and a cross-cultural comparison. International Journal of Intercultural Relations, 32, 505–514. doi:10.1016/j.ijntrel.2008.08.002
Park, C. L. (2005). Religion as a meaning-making framework in coping with life stress. Journal of Social Issues, 61, 505-514. doi:10.11/j.1540-4560.2005.0428.x
Pomerantz, A. M. (2010). Clinical psychology: Science, practice, and culture (2nd ed.). Thousand Oaks, CA: SAGE Publications, Inc.
Porter, M., & Haslam, N. (2005). Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. Journal of the American Medical Association, 294(5), 602-612.
Putnam, D., & Noor, M. (1993). The Somalis: Their history and culture (CAL Refugee Fact Sheet Series, No. 9). Retrieved from The Refugee Center for Applied Linguistics http://ethnomed.org/clinical/mental-health/somali-refugee-mental-healthculturalprofile/?searchterm=Solami%20Refugee%20Mental%20Health%20Cultural%20Profile
Robertson, C. L., Halcon, L., Savik, K., Johnson, D., Spring, M., Butcher, J.,… Jaranson, J. (2006). Somali and Oromo refugee women: Trauma and associated factors. Journal of Advanced Nursing, 56, 577-587. doi:10.1111/j.1365-2648.2006.04057.x
Roodenrijs T. C., Scherpenzeel R. P., & de Jong J. T. V. M. (1998). Traumatic experiences and psychopathology among Somalian refugees in the Netherlands. Tijdschrift voor Psychiatrie, 40(3), 132–142.
Rousseau, C., Said, T. M., Gagné, M., & Bibeau, G. (1998a). Resilience in unaccompanied minors from the north of Somalia. Psychoanalytic Review, 85(4), 615-637.
Rousseau, C., Said, T. M., Gagné, M., & Bibeau, G. (1998b). Between myth and madness: The premigration dream of living among young Somali Refugees. Culture, Medicine & Psychiatry, 22(4), 385-411.
Sack, W. H., Angell, R. H., Kinzie, J., & Rath, B. (1986). The psychiatric effects of massive trauma on Cambodian children II: The children, the home, and the school. Journal of the American Academy of Child Psychiatry, 25, 370-376. doi:10.1016/S00027138(09)60260-0
Scales, P. C., & Roehlkepartain, E. C. (2003). Boosting student achievement: New research on the power of developmental assets. Search Institute Insights & Evidence, 1, 1-10.
Schuchman, D., & McDonald, C. (2004). Somali mental health. Bildhaan – An International Journal of Somali Studies, 4, 65-77.
Shrestha, N. M., Sharma, B., Van Ommeren, M., Regmi, S., Regmi, S., Makaju, R., … de Jong, J. (1998). Impact of torture on refugees displaced within the developing world: Symptomatology among Bhutanese refugees in Nepal. The Journal of the American Medical Association, 280, 443-448. doi:10.1001/jama.280.443
Silveira, E., & Allebeck, P. (2001). Migration, ageing and mental health: An ethnographic study on perceptions of life satisfaction, anxiety and depression in older Somali men in east London. International Journal of Social Welfare, 10(4), 309-320.
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioural Medicine, 15(3), 194-200.
Steele, Z., Chey, T., Silove, D., Marnane, C., Bryant, R. A., & van Ommeren, M. (2009). Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. Journal of the American Medical Association, 302, 537-549. doi:10.1001/jama.2009.1132
Steele, Z., Silove, D., Bird, K., McGorry, P., & Mohan, P. P. (1999). Pathways from war trauma to posttraumatic stress symptoms among Tamil asylum seekers, refugees, and immigrants. Journal of Traumatic Stress, 12, 421-435. doi:10.1023/A:1024710902534
Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The Meaning in Life Questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53, 80–93. doi:10.1037/002-0167.53.1.80
Steger, M. F., Kashdan, T. B., Sullivan, B. A., & Lorentz, D. (2008). Understanding the search for meaning in life: Personality, cognitive style, and the dynamic between seeking and experiencing meaning. Journal of Personality, 76, 199–228. doi:10.1111/j14676494.2007.0484.x
Stutters, A., & Ligon, J. (2001). Differences in refugee anxiety and depression: Comparing Vietnamese, Somalian, and former Yugoslavian clients. Journal of Ethnic & Cultural Diversity in Social Work, 10, 85-96. doi:10.1300/J054v10n01_05
Sun, J., & Stewart, D. (2007). Development of population-based resilience measures in the primary school setting. Health Education, 7(6), 575-599.
Thabet, A. A., & Vostanis, P. (2000). Post-traumatic stress disorder reactions in children of war: A longitudinal study. Child Abuse & Neglect, 24, 291-298. doi:10.1016/S0145-2134(99)00127-1
Tiliouine, H. (2006). Measuring wellbeing in developing countries: The case of Algeria. Social Indicators Research, 75, 1-30. doi:10.1007/s11205-004-2012-2
Ungar, M. (2008). Resilience across cultures. British Journal of Social Work, 38, 218-235. doi:10.1093/bjsw/cl343
Ungar, M. (2010). Families as navigators and negotiators: Facilitating culturally and contextually specific expressions of resilience. Family Process, 49, 421-435. doi:10.1111/j.15455300.2010.01331.x
Ungar, M., Brown, M., Liebenberg, L., Othman, R., Kwong, W., Armstrong, M., & Gilgun, J. (2007). Unique pathways to resilience across cultures. Adolescence, 42(166), 287-310.
Ungar, M., & Liebenberg, L. (2009). Cross-cultural consultation leading to the development of a valid measure of youth resilience: The International Resilience Project. Studia Psychologica, 51(2-3), 259-268.
Ungar, M., & Liebenberg, L. (2011). Assessing resilience across cultures using mixed methods: Construction of the child and youth resilience measure. Journal of Mixed Methods Research, 5(2), 126-149.
Ungar, M., Liebenberg, L., Boothroyd, R., Kwong, W. M., Lee, T. Y., Leblanc, J., … Maknach, A. (2008). The study of youth resilience across cultures: Lessons from a pilot study of measurement development. Research in Human Development, 5, 166-180. doi:10.1080/15427600802274019
United Nations Development Program (UNDP). (2001). Human development report: Somalia. New York, NY: Author.
United Nations High Commissioner for Refugees. (2006). Protracted refugee situations: Search for practical solutions. In State of the world’s refugees: Human displacement in the new millennium. Geneva, Switzerland: Author.
United Nations High Commissioner for Refugees. (2010). Statistical yearbook 2009: Trends in displacement, protection and solutions. Geneva, Switzerland: Author.
United Nations High Commissioner for Refugees. (2011). Global strategic priorities. Geneva, Switzerland: Author.
United Nations High Commissioner for Refugees. (2012). Who we help. Retrieved from Author http://www.unhcr.org/pages/49c3646c11c.html
Waaktaar, T., Torgersen, S. (2010). How resilient are resilience scales?: The Big Five scales outperform resilience scales in predicting adjustment in adolescents. Scandinavian Journal of Psychology, 51, 157-163. doi: 10.1111/j.1467-9450.2009.00757.x
Wagnild, G. G., Young, H. H., Heilemann, M. V., Lee, K. A., & Kury, F. S. (2002). Resilience Scale. Nursing Research, 51, 175-182.
Warfa, N., Bhui, K., Craig, T., Curtis, S., Mohamud, S., Stansfeld, S., … Thornicroft, G. (2006). Post-migration geographical mobility, mental health and health service utilisation among Somali refugees in the UK: A qualitative study. Health & Place, 12(4), 503-515.
Werner, E. E., & Smith, R. S. (1977). Kauai’s children come of age. Honolulu: University of Hawaii Press.
Werner, E. E., & Smith, R. S. (1982). Vulnerable but invincible: A longitudinal study of resilient children. New York, NY: McGraw-Hill.
Werner, E. E., & Smith, R. S. (2001). Journeys from childhood to midlife: Risk, resilience, and recovery. Ithaca, NY: Cornell University Press.
Whittaker, S., Hardy, G., Lewis, K., & Buchan, L. (2005). An exploration of psychological well-being with young Somali refugee and asylum-seeker women. Clinical Child Psychology & Psychiatry, 10(2), 177-196.
Williams, C. L., & Berry, J. W. (1991). Primary prevention of acculturative stress among refugees: Application of psychological theory and practice. American Psychologist, 46, 632–641. doi:10.1037/0003-066X.46.6.632
Windle, G., Bennett, K. M., Noyes, J. (2011). A methodological review of resilience measurement scales. Health & Quality of Life Outcomes, 9, 8-25. doi:10.1186/14777525-9-8.
Windle, G., Markland, D. A., & Woods, R. T. (2008). Examination of a theoretical model of psychological resilience in older age. Aging & Mental Health, 12, 285-292. doi:10.1080/13607860802120763
Young, M. Y. (2006). Moderators of trauma in Somali mothers. International Journal of Psychology, 31(3-4), 324-246=
Appendices
Appendix A
Summary of Resilience Measures
| Name | Author(s) | Target population | Number of dimensions (items) | Description of the measure
|
| The Dispositional Resilience Scale (1) (USA/English) | Bartone, Ursano, Wright, & Ingraham(1989) | Adults | 3 (45) |
|
| The ER 89 (USA/English) | Block & Kremen (1996) | Young adults (18-23) | 1 (14) |
|
| The Connor-Davidson Resilience Scale (USA/English) | Connor, Davidson, & Lee (2003) | Adults (mean 43.8) | 5 (25) |
|
| Youth Resiliency: Assessing Developmental Strengths (Canada/English) | Donnon & Hammond (2007); Donnon, Hammond, & Charles (2003) | Youth (age 12-17 | 10 (94) |
|
| The Resilience Scale for Adults (Norway/Norwegian) | Friborg, Hjemdal, Rosenvinge, & Martinussen(2003) | Adults | 5 (37) |
|
| The Resilience Scale for Adults (RSA) | Friborg, Barlaug, Martinussen, Rosenvinge, & Hjemdal(2005) | Adults (mean age 22, 24, mid 30s) | 6 (33) | Same as above. |
| The Resiliency Attitudes and Skills Profile (UAS/English) | Hurtes & Allen (2001) | Youth (age 12-19) | 7 (34) |
|
| Adolescent Resilience Scale (Japan/Japanese) | Oshio, Kaneko, Nagamine, & Motoyuki (2003) | Japanese Youth (19-23) | 3 (21) |
|
| California Healthy Kids Survey- The Resilience Scale of the Student Survey (USA/English) | Sun & Stewart (2007) | Primary School Children | 12 (34) |
|
| The Brief Resilience Scale (USA/English) | Smith et al., (2008) | Adults (19-62) | 2 (6) |
|
| The Child and Youth Resilience Measure (CYRM) (11 countries/11 languages) | Ungar et al., (2007) | At risk youth (12-23) in different countries | 5 (28) |
|
| The Resilience Scale (RS) (Australia/English) | Wagnild, Young, & Heilemann (2002) | Adults (some 16-23) | 2(25) |
|
| Psychological Resilience (UK/English) | Windle, Markland, & Woods (2008) | Older adults | 2 (19) |
|
| Ego Resiliency (1) (USA/English) | Klohnen (1996) | Adults (18-48) | 4 (20) |
|
| Resilience Scale Adolescents (READ) (Norway/Norwegian) | Hjemdal, Friborg, Stiles, Martinussen, & Rosenvinge (2006) | Adolescents (13-25) | 5 (39) |
|
| Ego Resiliency (2) (USA/English) | Bromley, Johnson, & Cohen (2006) | Adolescents and young adults | 4 (102) |
|
Note: Reprinted from Windle, Bennett, & Noyes (2011)
Appendix C
Study Materials
Informed Consent
PRINCIPLE INVESTIGATORS
DESCRIPTION
You are invited to participate in a research study. The research will look at how Somali people live well when faced with difficulties. If you decide to participate, you will partake in an interview with a trained interviewer that will last about 60-90 minutes. The interview will be private and confidential.
PROCEDURE
First, the interviewer will explain the research to you, answer your questions, and ask for your permission to audio record the interview. Second, the interviewer will ask you some questions about yourself, like your age, religious faith, the name of any refugee camps you spent time at, your current refugee status, and how long you’ve been in the United States. Finally, with your permission, the audio recording will be started and you will be asked questions about how you managed to live well in Somalia, in the refugee camps, and in the United States despite the challenges you may have faced. Please note that the research team will transcribe the audio recording. Any identifying information will be removed from the transcription. Once transcription is complete, the recording will be deleted.
RISKS
You will be asked to think and talk about personal life experiences. Some people may feel an invasion of privacy or uncomfortable answering these questions and some may even feel distressed. If you feel very uncomfortable while answering questions, please tell the interviewer. If there is a question that you do not want answer, you do not have to respond. You may stop answering the questions at any time.
BENEFITS
There are no direct benefits from participating in this research. However, this study provides you the opportunity to teach professionals who work with Somali people in the United States and abroad about the strengths of Somali people. This information will be used to promote and improve well-being in Somali communities.
COMPENSATION
Your participation in this study is greatly appreciated! You will receive $20 for participating in this study, whether or not you complete the interview.
VOLUNTARY NATURE OF PARTICIPATION
Your participation in this study is voluntary. If you decide to participate, you may stop being a part of the study at any time. If you decide to stop being a part of the study, your answers will be returned to you or destroyed.
CONTACT PEOPLE
SIGNATURE
Your signature on this consent form indicates that you fully understand the above study, what is being asked of you in this study, and that you are signing this voluntarily. If you have any questions about this study, please feel free to ask them now or at any time throughout the study.
Signature Date
Printed Name _____________________________
A copy of this consent form is available for you to keep.
Demographics
To begin, I would like to ask you some questions about yourself. Please remember that all of your responses are completely confidential and for research purposes only.
______________________________________________________________________
|
Age: |
|
|
Gender: |
|
| Marital status: | |
|
Religious faith: |
|
|
Nationality: |
|
|
Refugee status: |
|
|
Length of residence in refugee camps: |
|
|
Location of refugee camp(s): |
|
|
Length of residence in the US: |
Key-informant Protocol
Complete Checklist Prior to Interview:
- Obtain written consent.
- Gather demographic information.
- Turn on both audio recorders.
Helpful hints for interviewer:
- Use a casual style; remember we are trying to learn about resilience and we are looking to gather rich, meaningful responses to the questions below.
- Ask follow up questions and make sure you understand what the person is telling you.
- Tell me more about…
- Give me an example of a time when…
Interviewer:
I’m going to ask you some questions about your life in Somalia and the United States. We are trying to learn about what helps people during times of difficulty. If any of the questions are confusing, tell me and I will try and ask you in a different way. Once I ask you the question, you can talk for as long as you would like, sharing your experiences as a Somali person. Any questions before we start?
Interviewer:
To provide a context for your answers, tell me a little bit about life in Somalia and your journey to the US.
Interviewer:
Explain what a Somali person needs to know to live well in Somalia?
Follow-up: How is this the same and different from what you need to know to live well in [insert refugee camp, or other intermediate location]?
How is that the same and different from what you need to know to live well in the United States?
Interviewer:
How do you describe a person who lives well in Somalia despite the many problems they face?
How is this the same or different from how you describe a person who lives well in [insert refugee camp, or other intermediate location]?
How is that the same or different from how you describe a Somali person who lives well in the United States?
Interviewer:
What does it mean to you when bad things happen?
What does it mean to your family or community when bad things happen?
Interviewer:
What kinds of things were the most challenging for you living in Somalia?
What kinds of things were the most challenging for you living in [insert refugee camp]?
What kinds of things are the most challenging for you living in the US?
Interviewer:
What do you do when you face difficulties in your life?
How do you make meaning of difficulties in your life?
Interviewer:
What does being healthy mean to you?
What does being healthy mean to your family or community?
Interviewer:
How do you keep healthy (mentally, physically, emotionally, and spiritually)?
How do others you know keep healthy (mentally, physically, emotionally, and spiritually)?
Interviewer:
Describe what gives you hope for the future?
Interviewer:
That was my last formal question. One of the most important parts of this research is to share what we learn with the Somali community and make the research useful to the Somali community. Before we finish the interview, can you think of any ways that this information could be made useful for you and the broader Somali community?
How would you suggest sharing what we learn with the Somali community?
Debriefing
PURPOSE
Thank you for participating in an interview with the Somali Resilience Project! The purpose of this interview was to learn about how Somali people live well when faced with difficulties. The information will be used to teach professionals who work with Somali people in the United States and abroad about the strengths of Somali people. You participation is highly valued.
CONFIDENTIALITY
The recording of this interview will be transcribed and any identifying information will be removed from the transcription. Once transcribed, the recordings will be deleted. Your personal information will be kept strictly confidential and stored and locked in a secure location to ensure your privacy.
FINAL REPORT
CONTACT
If you live in Minnesota:
- University of Minnesota Community-University Health Care Center: (612) 638-0670; http://www.ahc.umn.edu/cuhcc/
- Somali and East African Behavioral Health Clinic: (612) 767-0019; http://www.voamn.org/Somali-MH
If you live in Alaska:
- University of Alaska Anchorage Psychological Services Center: (907) 786-1795; http://www.uaa.alaska.edu/psych/services/
- Anchorage Neighborhood Health Clinic: (907) 257-4600; http://www.anhc.org/
IN APPRECIATION
You have received $20 in appreciation of your participation in this research.
Appendix D
Qualitative Data Codebook
| Somali Resilience Project Codebook-1 | |||
|
Definition of Resilience |
|||
|
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways. |
|||
|
Research Question |
|||
| How is resilience conceptualized in the context of Somali culture and the refugee experience? | |||
|
Guiding Questions |
|||
| What is health?
What are health-sustaining resources? How are resources navigated? How are resources negotiated? |
|||
| Code | Definition | Key Words | For Example |
| Context | Merged ‘Somalia’, Refugee camp’, ‘United States’, and ‘Nuanced context’ codes. Broadest level of coding with the purpose of categorizing data broadly by context. Should also capture “cross-context” or context-specific-comparison references, while eliminating context-neutral references. | ||
| Somalia | Reference to Somalia. | Somalia, East Africa, Africa in general (not specific location) | “Most of my childhood I was a nomad, I used to look after the camel. As a child we usually start with the goats, the baby goats, then you move onto the goats, then you move onto the cows, then you get to the camel. That’s the career ladder [chuckle].” |
| Refugee camp | Reference to refugee camp. Broadest level of coding with the purpose of categorizing data broadly by context. | Refugee camp | “Living well in a refugee camp, I mean that term to me… in a refugee camp you can never live well. There isn’t anything like that. You’re in a survival mode. So surviving is very important. And a person who is living well means they are surviving.” |
| United States | Reference to United States. Broadest level of coding with the purpose of categorizing data broadly by context. | United States, US, West | “The United States is a great country. There’s a lot of resource for people, but the resource need to be utilized. In America there’s a lot of resource that you cannot get maybe in the Third world.” |
| Somali Resilience Project Codebook-2 | |||
| Definition of Resilience | |||
|
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways. |
|||
| Research Question | |||
|
How is resilience conceptualized in the context of Somali culture and the refugee experience? |
|||
| Guiding Questions | |||
|
What is health? What are health-sustaining resources? How are resources navigated? How are resources negotiated? |
|||
| Code | Definition | Code | For Example |
| Individual
|
Reference to individual capacity for to navigate resources. | Personality, determination, optimism, confidence, intelligence, hard work, locus of control, skills, individualistic concerns, knowledge. | “…do no matter where you are at, whether you are in a refugee camp, whether you’re in United States, whether you are back home, determination is the key of your future. |
| Relational | Reference to family or other relations. | Mother, father, family, siblings, cousins, neighbors, clan, connections, and other one-to-one relations. | “Back home, really, we have a good family system. All relating to each other really and helping to each other…my cousin from my mother and my cousin from my father, and maybe my neighbors…” |
| Community | Reference to community. | Work, schools, Universities, mosques, community centers, organizations, education, educational resources, programs, and the interaction of such entities, community resources, government, laws. | “I try to teach my neighbors. Then after neighbors, we go by neighborhood, and then we go for our community, maybe the State of by the government.” |
| Culture | Reference to culture and cultural values. | Religion, values, ethnicity, language, dress/clothing, food, clan-structure, gender, generation (age), collectivistic concerns. | “As a Muslim person being healthy means is every morning you get up you should thank God. Yeah. So, I every morning that I get up and see the sun, or you know see myself breathing I should remember and thank God.” |
| Nuanced Context | Reference to nuanced contextual concepts. | Rural, urban, nomad, pastoralism, specific refugee camps, specific cities, physical environment (e.g., climate). NOT Somalia, Refugee Camp, US (broadly defined), climate, weather. | “…when you go there, it’s hot, very hot. The dust in your face, you’re thirsty, you cannot get water, because maybe the place, the shelter.” |
| Adversity | Reference to exposure to adversity. | Challenges, barriers, discrimination, financial concerns, trauma, rape, murder, acculturation stress. | “And the camp was not a fun place…really bad malnutrition. You can see children malnourished. You can see adults dying; nobody take care of them.” |
| Resources
|
Reference any sort of health-sustaining resource. | Social services, aid agencies, public assistance, food, water, medicine, health care, education, family as a resource, community as a resource, culture as a resource, opportunities, lack of resources. | The United Nations, they make food, like cornmeal, course meal, maybe make them like some traditional food whatever they have. They get oil, sugar and some basic food. |
| Outcomes | Reference to positive or negative outcomes. | Health outcomes, educational outcomes, work fulfillment, prevention, living “good life”. | “Basically I would say the education piece, the family, the faith, and those would be 3 markers of success.” |
|
Somali Resilience Project Codebook-3 |
|||
| Definition of Resilience | |||
|
In the context of exposure to significant adversity, whether psychological, environmental, or both, resilience is both the capacity of individuals to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being, and a condition of the individual’s family, community and culture to provide these health resources and experiences in culturally meaningful ways. |
|||
| Research Question | |||
|
How is resilience conceptualized in the context of Somali culture and the refugee experience? |
|||
| Guiding Questions | |||
|
What is health? What are health-sustaining resources? How are resources navigated? How are resources negotiated? |
|||
| Code | Definition | Code | For Example |
| Adaptation
|
Reference to adaptation. | Acculturation, assimilation, biculturalism, marginalization, general adaptation statements, including difficulties. | “They adjust there too despite the war. They get used to all these problems by adapting, getting guns.” |
| Charity | Reference to contribution (or giving back). | Charity, contribution to the community, feelings of usefulness, volunteering., giving back to the community, caring for others in need. | |
| Communication | Reference to communication and networks of communication. | Technology, oral communication, communication networks, advocating for personal and collective needs through verbal or written communication, language. | “…how to communicate with the people and improve my language, or how to contact my family, how to call them.” |
| Cooperation | Reference to cooperation and networking (process and outcome). | Cooperation, cooperative living and sharing, etc. | “We share everything. If you are rich, they make you poor, because you are sharing [laughter]. We don’t hold back. If you are poor, they will make you rich.” |
| Coping | Reference to coping with stress. | Prayer, meditation, staying calm, talking with others, problem solving as a coping mechanism, protecting oneself. | |
| Education | Reference to education. | ||
| Emotional expression | Reference to emotional expression. | Happy, cry, laughing, angry, expressions of emotion, feelings, thoughts, feelings, associations, distress. | “When I go there- my eyes used to cry a lot.” |
| Future orientation | Reference to focusing on the future and not dwelling in the past. | Moving on, next step, goals, vision of future. | “My question will be, what can I do about this happening? What could I do better? Or what could I prevent to happen next time?” |
| Gender | Reference to gender. | Gender roles, gender-oriented power dynamics. | And he said, “I think there was a mistake, you need to go back to the human resources, because we never hire any female before.” |
| Generation | Reference to generational concepts. | Elders, adolescence, youth, children. | “I think our parents do an amazing job keeping food on our table, maneuvering around the system to get public assistance, and housing, just put us through education…it’s the first generation who are coming over here, who fall in the gaps—who fall into drugs, alcohol, and other things.” |
| Health | Reference to health and well-being. | Physical, emotional, mental, and spiritual well-being; sickness; feelings of well-being, “living well”. | “So to keep healthy mentally and to keep healthy emotionally you must have a strong Iman [faith]. You must have a strong faith, and pray, and if you do that that emotionally, mentally, physically, that should all be taken care of.” |
| Hope | Reference to hope. | “My hope for myself is just focusing on the changes that the little kids make, little Somali kids… if I see positive changes in them then that’s my hope because I feel like they’re the only ones who can kind of change everything that we’re having right now in Somalia.” | |
| Migration
|
Reference to movement between locations. | Transportation, method of transportation, process of migration, movement, nomadic migration. | “… my mom, she used to go back and forth to the city [Nairobi], and get something, get maybe small clothes for the ladies then sell if over there [refugee camp]… So we used to go back and forth, the camp and the city.” |
| Navigation/negotiation | Reference to navigation and negotiation of resources. | Knowledge of resources, capacity to navigate toward resources, and process of negotiating for resources, problem solving as a process of negotiation of resources. | “You know the language, you know where to go; you know who to approach if you need help; you know the system and how it functions.” |
| Opportunity | Reference for various opportunities. | Employment opportunity, educational opportunity, business opportunity, work, | |
| Spirituality/faith | Reference to spirituality and faith as a component of spirituality. | Faith, spirituality, religious beliefs and practices, prayer, “god willing”, Inshallah, Iman. | “A high percent of Somali people we just trust God, and whatever came through to you it’s already been written.” |
| “That’s the general Muslim concept. As a Muslim community it is always Inshallah [God Willing], and to God we belong, and to him we’ll return. And hopefully something good will come out of whatever is going on.” | |||
| Survival | Reference to survival. | “At one point you gonna say, “How am I going to survive this minute?” In a refugee camp or displaced or whatever that journey was, at some points you cannot think tomorrow you can only think only that minute and say, “How I gonna survive this minute? This moment?” | |
| Zoo
|
Important concepts not captured elsewhere. | Discuss | |
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Psychology"
Psychology is the study of human behaviour and the mind, taking into account external factors, experiences, social influences and other factors. Psychologists set out to understand the mind of humans, exploring how different factors can contribute to behaviour, thoughts, and feelings.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: