Oral Cancer Symptoms, Types and Risk Factors
Info: 9378 words (38 pages) Dissertation
Published: 30th Nov 2021
Tagged: Cancer
Abstract
Although oral cancer is uncommon and attracts in little consideration, it positions twelfth among all cancers and constitutes the most life undermining of every single dental condition. The etiology of oral cancer is multi-factorial and like different sorts of cancer, the way to diminishing the suffering of patients and expanding their survival rate is early detection.
The worldwide increment in recurrence of oral cancer has intensified current research efforts in the field of anticipation and early discovery of this disease.
In spite of the fact that advances in the treatment of oral cancers have been made over the most recent four decades, benefits have not been reflected in mortality figures. In this way, essential counteractive action, for example, suspension of tobacco smoking and liquor utilization alongside early identification are fundamental control strategies to enhance the visualization for oral cancer [1]. In any case, it is pivotal to recognize pertinent hazard variables for contracting oral cancer before execution of counteractive action programs. Here, we survey the important writing and fundamentally assess the hazard elements for contracting oral cancer.
Contents
Objectives………………………………………………. 2
1. Introduction……………………………………………3
2. symptoms of oral cancer …………………………..…..9
3. Types Of Oral Cavity Cancer…………………………….10
4. Risk factors ………………………………………….….14
5. Early detection and prevention of oral cancer………… 19
6. clinic examination ……………………………………. 22
7. Self-examination and other examination ……………….27
8. Oral cancer diagnosis tests………………………….….28
9.Management………………………………………………30
10.conclucion ……………………………………………..35
11. References …………………………………………..38
Objectives
Early detection of oral cancer needs something other more than comprehension of the signs and side effects of illness. The procedure must be overseen successfully and dealt with delicately. Each individual from the dental team has a section to play and conventions ought to be created for effective delivery of:
- Standard examination of the oral cavity of patients.
- Management of recognized mucosal injuries with a fitting referral.
- Management of patients with ways of lifestyles that contribute to an increased risk of oral cancer.
The objective of this study is to develop clinical guidelines and realistic counseling for dentists in primary care who are now seeking to adopt best practices in oral cavity screening and case detection. Oral cancer mortality will be reduced only if the disease has been identified earlier, avoid delay in diagnosis, and treat it sooner. Increasing public awareness, continuing vocational education and improving health systems (referral), we believe, will help us achieve this goal.
Introduction
Cancer is the second for the most part normal reason for death in the Western world, after cardiovascular ailments [4]. Around the world, an expected cancer rate of around 10 million was accounted for the year 2010 [2], and 1 out of each 3 people is evaluated to experience the ill effects of cancer by the age of 75 years [4]. It is additionally assessed that 7.9 million individuals worldwide will bite the dust from cancer this year [2] , representing about 12% of passing around the world [2] . Late distributed appraisals of overall recurrence of the 16 noticeable cancers show that in creating nations with a high predominance of irresistible and nutritious sicknesses, cancer residue a noticable reason for death [2] . This may account somewhat for the present measurements whereby the greater part the worldwide occurrence of cancer is from the alleged creating nations, since an expected 70-80% of the worldwide populace lives in these territories [2]. The assessed yearly frequency of cancer extents from 48 to 225 for every 100,000 in creating nations ]2[ .
“Oral cancer” incorporates all malice beginning in an oral hole . Oral cancer positions the six in the general rate for the most 10 consistent cancer districts worldwide phenomenon and third in the creating nations [4]. There is furthermore a checked divergence in geographic event among the “height” and “lower” inescapability zones of the univrse, proposing main geographically differences in danger operators [3] [4]. The larger part of these operators have been perceived out of epidemiologic audits. For exact objectives , oral cancer is much of the time assembled with cancers of the maw as “oropharyngeal” cancer [11]. In the Westerner world, oral cancer is by and large incredible, and concerning each and every debilitating tumor, recurrence in the America and England ranges from 2 to 3% [1][11]. Relative rate of up to 5% while it has been represented America [10], and higher average have been represented the charged “high danger” domains of Europe to event comparatively moving with different money related social occasions inside these districts[3]. Around the globe, it is assessed that 300,000 people have been resolved to have oral cancer in 2010[2]. Of these, 126,000 have kicked the can from the illness [4]. In the United States alone, a normal 35,000 new cases of oral cancer will be resolved in 2009 to have a normal 7,500 resultant passing [1]. In the Asian , oral cancer is the most understood damage, speaking to around 33% of all malignancies inside the subcontinent [3][11]. Around 100,000 new cases are assessed to happen each year in those areas [11].
The peculiarity in the past disheartening experiences is that, notwithstanding the way that the oral melancholy and oropharynx are readily attainable to dental expert and specialists for routine checking and the biopsy of suspect bump that consistently give remarkable parts, early conclusion has been unpleasantly direct when differentiated and the promote early area of chest, colon, prostate cancers, and melanoma[12]. In this way, the passing rate from oral cancer as far back as three and a half deed has existed high (the greater part) despite new therapy modalities. On the other hand, there has been an amazing diminishing in death average for cancers of the chest, colon, prostate, and melanoma in the midst of comparable period [12] . valuation of the colonic mucosa, that demanded endoscopic checking for valuation of colon cancer, detect 36% of constrained colon cancers through America masses [12] . A vague rate of restricted oropharyngeal cancers are investigated without verbal through a comparable masses[12] .
This problem was expressively digested in a four deed-old generation highlight ” the poor figure of a sort of cancer, that represents astoundingly incredible open entryway for early treatment” [13][14]. The hindrance to premature assurance of the oral and oropharyngeal cancers, paying little mind to extended relentlessness as for dental authorities and oral specialists in their valuation of patients at peril, originates from the determination of old perfect models, and the nonattendance of an easily open decisive associate. Remembering the true objective to manufacture the premature ID of oral cancers, and by very active grow the survival rates of oral cancer patients, there is thus the necessity to perceive symptomatic checking formats that recognize early oral hazardous wounds with accuracy. Around 95% of oral cancers are assembled Physically as oral squamous epithelium [1] [2] [12]. Whatever remains of the 5% fuse like histological varieties as oral veracious carcinoma, Glandular cancer, Glandular squamous cells carcinoma, Mucous carcinoma, and Basal cell carcinoma.
Mucous cancers are malice of Saliva organ cause and, inside the oral opening, rise up out of small saliva organs, whereas Adenos Camus cancer are starting at now acknowledged to rise up out of the oral mucosa with bringing glandular changes through the tumors cells . Basaloid Psoriasis cell cancer , a tolerably as of late saw component, is an extraordinary histological with checked slant for the basis of tongue in spite of the supraglottic throat and Lower pharynx. Frequently fused into the scraps are roving cancer from nearby goals far away to the oral depression.
A number of these cancers can be avoided through way of life decisions that diminish unit hazard till the sickness. oral carcinoma , the concentration of that record, is a case of a to a great extent preventable sickness that in many occurrences can be connected to practices that incorporate long haul tobacco utilize, overwhelming utilization of liquor, and a horrible eating routine. extra 30,000 Americans will be determined to have oral carcinoma that year. till quite a while, the 5-year existence average for this gathering of carcinoma has been around half, notwithstanding propels in surgery, radiation, and chemotherapy. Notwithstanding unexpected passing, the dreariness related to the infection,And mental aches for patients, family and friends , and the money regarding costs make oral carcinoma a noteworthy general wellbeing concern. Accordingly, it is a height need to bring down the quantity of modem instances of oral carcinoma and additionally to lessen its dreariness and death-rate . It is a test that have been taken us to the year 2000, and past.
Counteractive action of oral carcinoma is basically imperative and can have been berefined in four paths , by [14] conception of circumstances , end results and adjusting related dangers [15] perceiving and controlling precancerous injuries; [16] setting up the most punctual conceivable finding and overseeing auspicious and fitting therapy; and [17] viably dealing with the complexities of therapy . A society of health organizations, drove by The Center of Disease Control and Prevention and The National Institutes of Health , have set up destinations, goals, and projects to complete the delegtion of decreasing dreariness and death-rate from oral carcinoma by 2000. As an initial step, the Centers for Disease Control caught a workshop in 1992, prompting this position.
The other step will have been a national gathering in August 1996, to put forward suggestions for open activity. those proposals and procedures will be incorporated and scattered by Centers for Disease Control and its accomplices. Finish on the duties took place by the people and gatherings amassed at the meeting will have been the following stride in doing the avoidance and premature location of oral carcinoma all the more a need in that nation. These foundation papers on oral cancer finish the principal arrange in this exertion. They have set up to overlay all parts of that sickness through specialists, speaking to a far reaching cluster of claims to fame and aptitude. The expectation was to deliver a reasonable, shortly, and genuine state report that returns coherently from the study of disease transmission to restoration. As the rate of oral carcinoma stays stable, the socioeconomics are variable , with a dynamic increment in ladies. Quite a few years prior the male and female proportion border 10 to 1; the proportion is presently around 2 till 1. that move is expected to a limited extent to expanding tobacco and liquor utilization among ladies, to some degree to expanding life span. Senior subjects now represent around 13% of the Americans populace, and the most of them are ladies. through known hazard variables, maturing seems to be the best relationship with Carcinogenicity.
The maturing procedure impacts Protoncogen items creating cell dysregulation among modifications in cell development and silencer albuminoidal . Henceforth, geriatrics go as an inseparable unit. Survey of histological sorts demonstrates that the considerable larger part of oral Malignant tumors are squamous cell cancer ; they emerge of the mucosa of the oral hole and are Calligraphy in starting point. Since those are surface lump, (except for salivary organs and the rare event of sarcomas), the area upgrades early identification.
Be that as it may, when numerous oral cancers are analyzed, they are as of now in cutting edge stages. In this way, endeavors to lessen oral cancer rate, grimness, and death-rate must be multifaceted and multidisciplinary. Understanding causative variables is a need as anticipation techniques are created. Maturing is a hazard figure outwardly an answer, yet viable control of two other hazard elements, tobacco and liquor utilization, is achievable and beneficial. Inquire about that creates a superior accommodating of Signs under cancerous cells will help both aversion and early identification, in this manner lessening grimness and mortality.
Investigations of healthful variables, chemoprevention, viral impacts, and ontogeny items likewise will be essential. Oral by mouth sores, specially Leukoplakias and Erythroplakias, happen as often as possible in grown-ups. Creating helpful ways to deal with their avoidance, expanding the exactness of determination, finding More biological signs for these sores, and enhancing their administration will be all the further objective of oral carcinoma control.
Along those lines, premature limitation joined with favorable therapy have been keeping on being basal for lessening the gloom and death-rate related this disease. In the meantime, clinical studies revenue in the utilization of surgery, radiation, and chemotherapy to promote existence ranges . Tragically, modern, extra forceful methodologies orderly transfer more nuisance.
The individual satisfaction for both the individuals who realize a decrease and the individuals who might live for a time frame with stable tumors is a noticeable worry. modification in splutter or taste, huge torment, oral and dental pollution , Mucous membranes and bone molder, and trouble with the rumination, nip , and speak may earnestly hinder patients and over and over lessen their personal contentment to an awkward scale. encore is essentially mandatory and ought to be counted at the era of therapy arranging.
2. Symptoms
Signs mouth cancer may include:
- A sore that doesn’t recuperate.
- A sore that drains.
- A development, knot or thickening of the skin or covering of your mouth
- Baggy teeth.
- Badly fitting dentures
- Pain tongue
- Jowl pain or solidness
- Difficult or excruciating chewing
- Difficult or excruciating swallowing
- Sore throat


3. Types Of Oral Cavity Cancer
1. Tongue Cancer
The tongue is a common spot where oral cancer develops, according to the Oral Cancer Foundation, so be sure to pay attention to this area. Changes in the appearance of your tongue, like bumps or swollen areas, are often signs of an issue. Thick, white patches, as well as red spots or sores on the surface of your tongue can also indicate leukoplakia – a condition that sometimes progresses to cancer – and should be evaluated by your dentist. Luckily, precancerous or cancerous patches of tissue can be surgically removed before they spread further.

2. Gum Cancer
Cancer can also develop on your gum tissue, so stay alert for changes that include bumps or thick, swollen areas along the gumline. If a suspicious tissue is found when your dentist examines your gums, a biopsy will be performed to verify it. A biopsy that shows the presence of cancer may then allow you to undergo further treatment that includes surgery or chemotherapy. On the other hand, if no cancer is found, your dentist may diagnose you with a certain stage of gum disease that warrants using Colgate Total® Mouthwash for Gum Health.

3. Throat Cancer
Cancer can develop in the soft tissues of your throat such as your voice box or vocal cords. People with throat cancer may notice changes such as lumps or swellings in the back of their mouth, but the signs can also be more vague, such as a sore throat, hoarseness or difficulty swallowing. According to NIH, if these signs don’t get better within a week or two, you need to see your dentist. Throat cancer is diagnosed with tests such as biopsies, x-rays or CT scans. If cancer is found, it can be removed with surgery or treated with radiation therapy.
4. Jaw Cancer
Malignant tumors are associated with many forms of cancer, and as a result, can form inside or on your jawbone. The University of California finds they sometimes produce symptoms such as lumps or thickening of the gum tissue, so it’s important to distinguish between jaw cancer and periodontal disease. This cancer can also make it hard for you to chew and swallow due to jaw pain, stiffness, a sore throat or even moderate hoarseness – all of which are possible symptoms. Like gum cancer, you may need to undergo tests such as CT scans, biopsies or MRI scans of your head to allow your dentist to see the infection. If a cancerous tumor is found, it can be surgically removed, and you may also need chemotherapy or radiation therapy during this process.
5. Lip Cancer
Basal cell carcinoma and squamous cell carcinoma, two types of skin cancers, can actually occur on your lips – which technically belong to your oral cavity. The lips are exposed to a lot of sunlight during the day and are often not protected by sunscreen as much as the Skin Cancer Foundation recommends. Signs of lip cancer include sores on your lips that don’t heal, swelling of the lips or general lip pain. If your dentist diagnoses you with lip cancer, you may need Mohs surgery, an effective skin cancer treatment for removing basal and squamous cell carcinomas with the use of a microscope and it has a high cure rate.

4. Risk factors
Tobacco
All various of smoking, tobacco, cigarettes, and smokeless weed have been involved in the development of oral cancer. Whereas smoking causes the highest risk for oral cancer of the tiers of the mouth also, it is linked with an increment risk for all locations of oral cancer. smoking is responsible for 90% of oral cancer death in the male.

Alcohol
Alcohol utilize is the second major risk factor for the expansion of oral cancer. Regard to non-Smoker it is the main risk factor. Over 30 grams of alcohol a day, the risk linearly rises with the amount of alcohol used.

Chewing tobacco
Addition to smoking, the utilize of chewing production like betel nut, dipping tobacco and snus, raises the risk for oral cancer; these productions are socially accepted in Asia, Pacific Islands, and India.
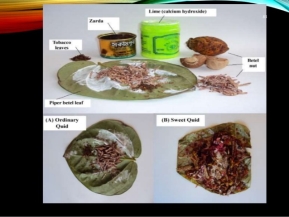
Shammah
Shammah, a classic smokeless tobacco usage in the Arabic Peninsula, has a historic association between the spread of leukoplakia and the diurnal duration of Shammah use in a potion-following manner.
Marijuana
The carcinogenic characteristics of marijuana smoking are like these of tobacco. Marijuana may react with mutagen sensibility and other risk factors to raises the risk of head and neck cancer.
Poor nutrition
Nutrition deficiencies, especially of Vitamin C, vitamin E, vitamin A, iron, selenium, and folate and other effect components have been related to raised risk of oral cancer. interference studies wherever regime has been completed have shown several useful effects on Pre-cancer circumstances and decrease the risk oral cancer, but moreover, work into the regime and the function of Chemical prevention in oral cancers is necessary.
UV light
Solar radiation is the main risk factor for lip carcinoma. The main majority of lip carcinoma happens on the lowest lip and a lot of patients have outdoor jobs where exposition to sunlight raises. Lip carcinoma is more popular in men three times than women who may have the impact of career, tobacco, and exposition to sunlight.
Irritation
Though it has been proposed that chronic irritation to the lining of the mouth from badly fitting or deficient synthetic teeth may be a risk factor for oral cancer, the majority of researchers have shown no engagement.
Dental plaque
Multi-supergiveval microbial dental plaque is a probable separate risk factor, as it owns Interaction with mutation related with saliva, and thus oral health may be a contributing factor in the development of oral cancer.

Rinse mouth
Ethyl alcohol is inserted to rinse the mouth as a dissolvent for other components, as a preservative. Oral cancer was not Statistically linked with oral utilize in alcohol or smoking users. actually, there is sufficient clinical clue to propose a relation between ethyl alcohol found in mouth rinsing and oral cancer.
Candidiasis
Polycardinocytosis of autoimmune ovaries an autosomal recessive disease related to a limited T-lymphocyte defective, and especially common in Finland, it appears to favor the increase of candida albians and prepare for chronic mucositis and oral cancer.

Diabetes
The molecular basis of the presumed association of diabetes with esophageal cell carcinoma may include epidemiological studies of insulin receptor substrate 1 and kinase adhesion coordination.
Free radicals
Free radicals like reactive oxygen types and reactive nitrogen types can act as initiators and providers in Cancer, whereas antioxidants extend care against Cellular and molecular harm raised by reactive oxygen species and reactive nitrogen types. The rise in reactive oxygen types and reactive nitrogen types may have been the event that produces the consuming and decrease of Salivary anti-oxidant, thus And explained the oxidative harm to DNA and proteins, possibly enhanced oral cancer.
Viruses
The role of viruses is still unclear. Proof may be stronger for high-risk human papilloma viruses. Studies show the raised risk of oral cancer in women with cervical cancer suggesting a common non-smoking risk factor, like human papilloma viruses: oral HPV transmission is one possibility. A recent multicentre status study showed that HPV-16 infection increased the risk of oral cavity cancer, especially pharynx. The role of infection with the Epstein-Barr virus and herpes simplex virus remains uncertain. The role of herpes simplex virus, HSV-1 and HSV-2, was also studied as a popular agent with tobacco, alcohol, or HPV-16. In a study using the mysterious logic technique.
Family history
The family history of oral cancer is a risk factor. Head and neck cancer patients display the raised susceptibility to chromosome infection.The study of the cDNA group and specific genes such as keratin 17 and 19, laminin-5, coenoxin-26 and endothelial vascular growth factor were also utilized differential expressed in head and neck tissue in doubt, with respect to normal tissues .
5. Early detection and prevention of oral cancer
Oral cancer is ranked among the main 10 cancers in the world. Oral squamous cell carcinoma constitutes over 95% of oral cancers. The hazard elements for Oral squamous cell carcinoma are notable. Tobacco and liquor being the real causes make the disease preventable. Information uncovers that exclusive around half of the patients survive the infection more than 6 years. In spite of advances in treatment modalities over past decades, a significant change in anticipation is not accomplished. This is owing to the inability to identify little sores and possibly dangerous injuries early, which blocks effective treatment. Thusly, early detection is the way to enhance survival rate in oral cancer patients.
Early detection is conceivable through screening programs and by utilizing specific symptomatic guides and biomarkers. Although broad research and clinical utilization of analytic guides and biomarkers are rising, they need viable achievability when connected to bigger populace at hazard and low financial gatherings. A current precise survey on screening projects and preventive measures on oral cancer infers that deliberate visual oral examination by a clinician is by a wide margin the most well-known strategy for screening. Taken a cost-effectiveness and increase its spread. Perceivability of the sore might be improved by utilizing extraordinary dyes.
A group randomized control revealed an affectability of 68.4% for the visual examination in recognizing oral cancer. They presumed that the individuals who cling to rehashed screening rounds show a maintained diminishment in oral cancer mortality, along these lines highlighting the significance of populace based screening programs focusing on tobacco and additionally liquor users.
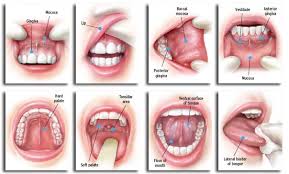
The National Institute of Dental and Craniofacial Research and World Health Organization recommend that screening for oral cancer ought to include a methodical visual examination of the oral pit and palpation of the tongue, floor of the mouth and provincial lymph hubs. On the off chance that any variation from the norm continues for over 3 weeks, then it requires a re-assessment and ought to be considered for biopsy. Screening might be focused at high hazard gatherings or shrewd, that includes individuals who go to health services for different reasons or a populace in general in view of statistics.
In opposite, an audit by the US Preventive Services Task Force on the proof of efficacy and accuracy of oral cancer screening programs uncovered insufficient confirmation on the analytic precision and benefits of oral cancer screening in asymptomatic grown-ups. US Preventive Services Task Force has in this way prescribed guiding to avoid tobacco utilize and to diminish liquor abuse. Unavoidably high-hazard bunches, for the most part, have a place with lower financial gatherings, who minimum go to the dental centers or use other health services, subsequently restricting an opportunity for visual examination by a clinician.
Less than 25% of subjects thought about tobacco or liquor as hazard components for oral cancer. This reflects the insignificant attention to oral cancer among the overall population. To defeat this essential issue, leaflet containing cancer data was utilized, which brought about a significant bring up in the information level of overall population, subsequently lessening persistent piece of delay. Therefore mass screening or health instruction for oral self-examination moves toward becoming crucial.Further, a postponement of 4-6 weeks is seen in the analysis due to absence of knowledge or absence of preparing among health experts, which requires a widespread preparing program for wellbeing experts to recognize early cancerous changes of the oral mucosa.
Diagnostic guides, for example, light-based detection frameworks are under broad research, however up until this point, controlled reviews have demonstrated no encouraging outcomes. They can be adjunctive to clinical examination in distinguishing cancerous or possibly threatening lesions. Biopsy still remains the highest quality level in definitive conclusion of suspected lesions. Since oral cancer is preventable, lessening in hazard consider seems, by all accounts, to be the most eective intends to decrease cancer grimness and mortality. Consolidated effect of liquor and tobacco is multiplicative or more prominent than multiplicative in most studies. Dentists and dental auxiliary personnel can lead tobacco discontinuance directing. Smoking end demonstrates a half decrease in danger of oral cancers inside 6 years.Currently, health instruction, prompt screening and Advising vulnerable groups is the key to early detection and screening.
6. Clinic examination
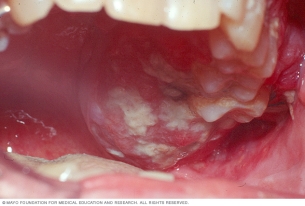
Oral Squamous Cell Carcinoma shows diverse clinical viewpoints which are connected with the area of the tumor, advancement time, precancerous injuries and hazard elements. The most regular clinical perspectives are: tumor, ulcer, vegetans, verrucous and blended structures, for example, ulcerous-vegetans or verrucose-ulcers (Boring et al., 1994). The diagnosis of early injuries, for example, in-situ or microinvasive carcinoma, clarify to a real challenge for health experts. Leukoplakia, erythroplakia or erythroleukoplakia are the most incessant clinical sides, which may show Surface eroded areas. Chorion invasion might be Suspected pupillary can be suspected when consistency is increased on observing.
The previously mentioned sores are asymptomatic, tend to keep their size, may indicate changes in the surface and don’t react to local medicines. The lesion can advance and create as an exophytic, unpredictable lobulated sore or embrace an endophytic development design portrayed by a discouraged ulcer with grayish-white edges, lifted and indurated borders and an infiltrated base.As a rule, lesions are asymptomatic; pain seems just when muscles or nerves are invaded at advanced stages of the disease. (Neville et al., 2002; Silverman et al., 1998), the lip is the most well-known area of oral squamous cell carcinoma.
In such cases, patients are probably going to counsel a doctor or a dermatologist while in instances of tongue tumors, the dental specialist is more frequent.The paramedial region of the sub-par lip is the regularly district influenced by lip cancer though the most prevalent precancerous lesions are actinic chronic cheilitis. Oral squamous cell carcinoma most regular center appearances are the loss of shallow tissue, disintegration, ulcers (Fig.1) and infrequently exophytic formed lesions: keratotic, verrucous or vegetant, with tumorous or “skin horn” sides(Neville et al., 2002; Silverman et al., 1998). Perpetual presentation to the sun produces in influenced patients an alteration of the state of the lip called lip everted or “lip on balcony”.
A critical atrophy of the vermillion range with scales that don’t tend to shed and along these lines gather to shape keratosis can frequently be watched. This kind of sores substitutes with white injuries and erythro-leukoplakia ranges that are inclined to splitting, disintegration or ulceration which are called actinic cheilitis. Lip cancer grows gradually and in cutting edge stages it can stretch out to the edge of the mouth or to the gingiva. It can likewise create metastatic lymph hubs in submental and submandibular zones (Grinspan, 1983) .

The paramedial area of the inferior lip is the most often region affected by lip cancer whereas the most prevalent precancerous lesions are actinic chronic cheilitis. OSCCs most common clinic manifestations are the loss of superficial tissue, erosion, ulcers (Fig.1) and occasionally exophytic shaped lesions: keratotic, verrucous or vegetant, with tumorous or “skin horn” aspect .Lateral border of the tongue and ventral surface of oral cancer are typically gone before by traumatic injuries brought on by sharp edged teeth, by gravely situated teeth or by maladjusted dentures that incessantly rub the mentioned areas. Ulcerated structures are the most much of the time observed, see Fig 2, trailed by exophitic tumor, which by and large produce pain to the ear. In the ventral region, ulcer-vegetant or blended structures prevail.
Tumors on the dorsum are by and large related to lichen planus or to leukoplakia sores. They are clinically noticeable as ulcerated structures have a tendency to develop the surface as opposed to go further into it. The parallel border of the tongue and the floor of the mouth consolidate to frame a shoeshaped district in the oral mucosa that was portrayed as very unsafe for cancer improvement and furthermore as a bad prognostic zone. These tumors have a tendency to advance towards the ventral side and to the floor of the mouth. There were 50% of the patients have lymph hubs. when the lesion has more than 3 cm, lymph hubs are available in 80% of the cases. Tumors located in the anterior half of the tongue more often than not prompt lymphadenopathy in the suprahyoid area while those situated in the back half prompt submaxillary, carotid and lateropharyngeal hubs. Contralateral hubs are more than from tumors in the ventral surface and floor of the mouth.

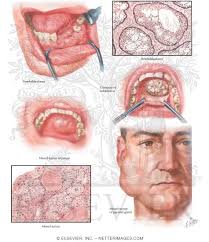
Chronic provocative procedures would discharge genotoxic arbiters that would animate the gathering of hereditary deformities prompting the presence of dangerous cells. In its underlying stage, gingival carcinoma resembles a red or/and white spot somewhat vegetant, stretching out at first glance because of the resistance offered by the periosteum (Fig 3). As oral cancer advances, it embraces a tumoral shape, it might attack the bones, loosening of teeth and cause pain or trismus. Its encouraging through the lymph influences the submental and carotid areas, these ones turning into the most widely recognized two-sided metastases. The antero second rate injuries advance towards the floor of the mouth and to the ventral side of the tongue. In the event that the tumor is situated in the back zone, it attacks the floor of the mouth and the masticatory muscles.

Most buccal mucosa is portrayed by creating on previous lesions. The leukoplasiform and erythroplastic structures are normally seen in the front some portion of the buccal mucosa while in the back one it is all the more regularly optional to traumatic sores or lichen planus. One of the main indications of the change is the induration of erythoplastic lesions that have a tendency to build up an exophytic aspect as they develop (Fig. 5). This sort of oral cancer once in a while exhibits ulcers though separated histopathologic structures are predominant. when oral cancer shows up in the third of the buccal mucosa, it as a rule presents itself as endophytic or ulcers; undifferentiated histological sorts is the most regular that have a more bad anticipation than in the front third. The influenced hubs are for the most part arranged in the submaxillary zone and less frequently in the cervical or facial ones .

7. Self-examination and other examination
Despite the fact that mouth self-examination utilizing a mirror has been assessed as a screening test in a few reviews , regardless of whether it could prompt decreases in oral cancer mortality is not known. There is insufficient proof to suggest the routine utilization of other oral screening tests, for example, toluidine blue recoloring, glow, tissue fluorescence imaging, tissue fluorescent spectroscopy, and salivary examination and cytology for primary screening of oral cancer.
It’s imperative to learn how to perceive the typical healthy state of your mouth with the goal that you can recognize anomalous conditions and report anything uncommon to a dental expert or a medical specialist.
- Look at yourself in the mirror – both sides of your face and neck ought to appear to be identical.
- Look at the skin on your neck and face for any adjustments in shading, moles that have changed, protuberances or wounds.
- Feel both sides of your neck delicately with your fingertips to help identify protuberances, knocks and sore spots.
- Gently put your finger over your “Thyroid cartilage” and swallow. It ought to climb and down, not to the side. Report any dryness that doesn’t clear up inside two weeks.
- Remove any dentures or machines from your mouth.
- Check within your mouth first by utilizing an electric lamp, then by putting the little mirror in your mouth, if you can do this.
8. Oral cancer diagnosis tests
Biopsy
If that any anomalies are found amid the test, a little tissue sample, or biopsy, normally is taken. This biopsy is critical, as it is the main beyond any doubt approach to knowing whether the unusual range is cancer. A biopsy might be acquired by:
Brush biopsy or exfoliative cells
This generally new kind of biopsy is easy and does not require a sedative. The dental specialist or specialist turns a little solid swarmed brush on the territory, bringing on scraped area or pinpoint dying. Cells from the range are gathered and inspected under a magnifying lens by a pathologist. In the event that outcomes are uncertain or indicate cancer, an incisional biopsy will be finished.
Anatomical biopsy
This is the conventional, most regularly utilized kind of biopsy. The specialist or dental practitioner surgically evacuates part or the majority of the tissue where cancer is suspected. More often than not, this procedure is finished in the specialist’s office or facility under local anesthesia. However, in the event that the tumor is inside the throat, the biopsy might be done in an operating with general anesthesia.
Fine-needle-yearning biopsy (FNA)
This kind of biopsy regularly is utilized if a patient has a protuberance in the neck that can be felt. In this methodology, a thin needle is embedded into the range. Then cells are pulled back and examined under a magnifying lens.
Reproduction of mucus
A blue dye called toluidine blue O is connected to the range where cancer is suspected. If any blue areas stay in the wake of rinsing, they most likely will be explored with a biopsy.
Chemiluminescent light
After you wash your mouth with a mild acid solution, your mouth will be examined with a unique light. Sound cells don’t mirror the light; cancerous cells do.
Imaging tests
which may include:
- computed axial tomography scans
- positron emission tomography scans
- magnetic resonance imaging scans
- Chest and x-ray teeth
- Barium ingestion : Also called an upper gastrointestinal arrangement, this set of X-beams of the throat and stomach might be utilized to search for different cancers and determine how well you swallow.
- Endoscopy
9. Management
The choice about the adequate treatment for every patient ought to be made by an interdisciplinary committee of experts in head and neck tumors. The decision of treatment to a great extent relies on upon the site and phase of the ailment and on the general wellbeing status of the patient. Early phases of intraoral cancers are probably going to be cured by surgery or radiation treatment. The decision of the sort of treatment is controlled by the expected practical and corrective outcomes and by the accessibility of the specific skill required from the specialist or radiation advisor for every patient. Propelled tumors (stages III and IV) are for the most part treated by surgery, trailed by radiation treatment.
The treatment for head and neck cancers, particularly those including the oral cavity, has changed over the most recent 20–30 years. It is currently broadly acknowledged that for cutting edge oral cancer tumors, surgery consolidated with radiation treatment has a superior result than if just a single of those modalities is utilized. In spite of the fact that the effect of neo-adjuvant chemoradiation may expand survival, it might likewise build morbidity considerably.
It merits saying that present appearance of technology connected to cancer medications has fundamentally enhanced the personal satisfaction of oral cancer patients.However, there are just a couple of information with regards to the length of survival in connection to new gadgets, for example, gamma beams, electrons, protons and nuclear cores, tridimensional, stereotactic, Modulated Intensity Radiotherapy and Image-Guided Radiation Therapy. The new technology enables the expert to better change radiation to the tumor, in this way decreasing the harm dispensed to the encompassing solid tissues, particularly major salivary organs and maxillaries.
Local radiation therapy is a still utilized asset; it requires the separation of the radiated patient and it ought to be completed by exceedingly experienced experts. Disregarding all the previously mentioned developments, the event of complications high, which would definitely postpone the standard remedial conventions. This reality, thus, would make patients inclined to repeat or to metastases.
More Complications of oral cancer
All treatments realted to manage oral cancer and also with head and neck cancers negatively affect the patients, particularly on their oral cavity; a few entanglements can emerge because of direct harm to oral tissues or to indirect regional or systemic toxicity. Also, dental care is viewed by numerous patients as a low need in their treatment. Shockingly, 95% of the treated patients were found to have dental maladies, for example, caries, periodontal sicknesses or sepsis. The variables that impact intensity and duration of oral damage are: the medicinal and dietary status of the patient, tobacco and liquor utilize, oral cleanliness and dental status, past surgical intercessions, and the showed radiation treatment.
Surgical risks and complications
Surgical administration of intraoral sores commonly incorporates both the essential sore and cervical lymph nodes. In a perfect way, surgery is chosen when permanent control of the tumor is looked for. The tumor organizing is fundamental to decide if just surgery is demonstrated or whether radiation or chemotherapy might be required later. The dangers and continuations of surgery fundamentally rely on upon the degree of the tumor and its relationship to contiguous oral structures.Spin-offs may incorporate disorders in speech and swallowing, torment, limitations in oral motor function; diseases, enteral nourishment, facial, neck and shoulder breakdown, disturbances in mental health, fibrosis, restorative deficiencies and bone injuries. Amid resection of oral cancers, teeth and their supporting bone are frequently removed. It is important to supplant missing components. A few patients may require an intraoral prosthesis for obturation of a velopharyngeal shortage or to reshape and enlarge the shapes of a resected hard palate.
Possible oral manifestations of radiotherapy
Patients that get radiation treatment in the oropharyngeal territory for threatening tumors may experience radiation treatment for 7 weeks with measurements going up to 8000cGy, contingent upon tumor sort and area. Radiotherapy is related with reactions that differ in force and term and are subject to a few variables. Not all patients will encounter every conceivable difficulty but rather they ought to know about the potential dangers. chronic complications in the short and long haul have been considered.
Lack of saliva amid the first week of radiation treatment adds up to 40-50% of the typical salivation stream. Following a 7-week regular treatment, it abatements to 10%. Lack of saliva subjective side effect xerostomy infers a few different indications like dysphagia, dysgeusia, dysosmia and speech challenges. Xerostomia achieves an adjustment in oral microflora and, as a result, cariogenic microorganisms streptococos mutans y lactobacilos prevail in the salivation, causing on caries and periodontal maladies.
The oral mucosa becomes soft, irritable and susceptible of fungal infections (candidiasis) and inflammations. Recently, preventive measures to decrease the effects of radiation induced xerostomy have been widely studied. To begin with, patients should give up tobacco, alcohol and spicy, too hot, too cold or too hard foods and replace them by soft and moist nutrients. Secondly, they should be advised to be well hydrated and to use saliva substitutes. Salivary gland tissue does not recover from high doses of radiation.
The quality and amount of spit is forever changed. Taste misfortune and adjustments may start with the initial 300-500 cGy. Following three weeks of treatment, it takes 600-9,000 times typical convergences of taste stimulant to evoke an ordinary taste reaction. Taste keenness levels for the most part come back to ordinary inside 2-11 months taking after fruition of treatment, if sufficient salivation is accessible .Both mucositis and diminished salivary flow may add to taste adjustment. Mucositis: Oral mucositis is the irritation that happens in the oral epithelium subsequently of antineoplastic medicines, for example, radiotherapy, chemotherapy or bone marrow transplant which are extremely frequent in these medications.
Not exclusively do the results of the irritation influence the personal satisfaction of the patient yet it can likewise mean an impediment in the use of the treatment, and an expansion in healing facility length of stay and therapeutic costs. Radiation-actuated mucositis relies on upon the ingested radiation measurements, fractioning, conveyance methodology and delicate tissue status. Other compelling patient-related factors are age, sex, wholesome condition, oral microbiota, salivary stream and aggravation among others. The investigation of the degrees of seriousness of oral mucositis has yielded distinctive outcomes originating from differing research focuses. This constitutes a noteworthy deterrent for the investigation of mucositis. The absence of a uniform orderly approach embraced for its assessment by methods for oral examination makes it hard to survey its results.
Conclusion
Oral cancer constitutes the most life threatening of all dental condition. Shockingly, most harmful oral tumors are not identified until they are in cutting edge stages. Fundamentally, this poor result is identified with the majority of patients exhibiting at an effectively propelled phase of illness at the time of diagnosis. Despite the fact that the biopsy study is key, it is an indicative technique with restricted affectability where a standout amongst the most vital elements of cancer has re-emerged.
Over the most few years, the enthusiasm for new diagnostic and prognostic methodology and to monitor patients in oral precancer and cancer has re-risen.
Besides, various molecular- demonstrative markers have been utilized to distinguish the nearness of oral cancer with fluctuating degrees of affectability and specificity. In any case, still, the absence of particular tumoral markers display in every threatening lesion of the oral cavity.
A multifaceted approach that integrates health instruction, tobacco and liquor control, early detection and early treatment is expected to lessen the weight of this prominently preventable cancer. Step by step instructions to achieve this is known; incredibly, it has not been connected in many nations, and not in the slightest degree in the high-burden nations.
Oral cancer usually occurs in men from a low financial institution who smoke and spend liquor. Patients continue to be shocked in presenting with late stage patients. Oral examination is a non-intrusive primary test for its application, it has the same susceptibility and privacy as those well-established cervical cancer screening programs, and it is most likely to be financially savvy when communicating to people a great opportunity in the West’s civilization. Without any formal screening project, dentists and GPs can provide the best services to these high-risk patients by performing oral vertebral screening and guiding these patients to build their interest in early signs and indicators of oral cancer.
Enhancing awareness among the overall population and essential care experts, putting resources into health administrations to give screening and early finding administrations for tobacco and liquor users, and giving satisfactory treatment to those determined to have intrusive cancer are fundamentally imperative oral cancer control measures. Imaging, histopathology, cancer surgery and radiotherapy framework and administrations, prepared experts, and the accessibility of chemotherapeutic operators are insufficient in numerous, truly bargaining early detection and ideal treatment.
As this part has illustrated, notwithstanding, these are moderate and practical. Most patients, ignoring the underlying indications, go to the discussion at cutting edge oral cancer stages. Pre-threatening injuries may show up 11 years before the underlying oral cancer indications. Despite the fact that the carcinoma might be preventable through treatment of pre-cancerous injuries, numerous dental practitioners and family doctors are not performing out the opportunistic oral cavity exams. Oral cavity cancers can be recognized effortlessly with a straightforward oral examination, yet contrasted with cancers that include more intricate screening tests, the rate of early finding has not enhanced after some time. oral cancer is identified with preventable hazard components. Along these lines, we emphatically advocate that specialists ought to demoralize every one of their patients from smoking and drinking too much. Besides, serious open advancement and instructive battles are basic to build quiet awareness . Dental experts have an imperative part both in essential anticipation of oral cancer – by inciting sound ways of life and in auxiliary counteractive action by recognizing oral cancer or its antecedent injuries at early stages.
References
1. Jemal A, Seagall R, Ward E et al. Cancer Statistics, 2008. Ka Cancer J Klein 2008; 58: 71-96. Sargiran K, Martoma H, Savaffy CM, Vivalte MM, Tyronin O. Survival after diagnosis of oral cavity cancer. By J Oral Maxilovac Sorg. 2008; 46: 187-191.
2. Jemal A, Siegel R, Xu J, Ward E. Kanser Statisticch, 2010. K. Kanser J Klein 2010; 60: 277-300.
3. Johnson Nu. Global view of cancer epidemics of oral cancer. In oral cancer: detection of patients and pests at risk, ed. Johnson, N. 1991. Ch.1. Cambridge: Cambridge University Press.
4. Johnson no. Tobacco use and oral cancer: a global perspective. J Dent Edok 2001; 65: 328-339.
5. Joseph your. Oral cancer: prevention and detection. Med Brink Praktion 2002; 11 (Sobel 1): 32-35,
6. Jovanovic A, Choltin E, Costins Begay, et al. Tobacco and alcohol related to the anatomical site of oral squamous cell carcinoma. J Oral Pathul Mead 1993; 22: 459-462.
7. Kato I, Nomura AM. Alcohol in the causation of upper gastrointestinal cancer in the gastrointestinal tract. R. J Kanser Ural Uncol 1994; 30B: 75-81.
8. Kelly AB. Spasm at the entrance of the esophagus. Brooke R Suk Med 1919; 12 (Laringol Sickt): 235.
9. Parkin cm, Lara E, Muir pussy. World Frequency Estimates of sixteen major cancers in 1980. International Journal of Cancer 1988; 41: 184-197.
10. Batsakis GG. Head and Neck Tumors, Clinical and Pathological Theory, Second Edition 1979. 6, pp144-146. Baltimore: Williams Wilkins Company
11. Daftary Duck, Morty Bare, Ponsel Robb, Gupta Bessie, Mehta Ves, J. Bendburg. Oral Squamous Cell Cancer, Tropical Diseases in the Tropics, Editor Patboh Sere, Wilson Dess, Daftari Duck, Johnson Nu 1992. Ch. 37, b. 429-448. Oxford: Oxford University Press.
12. Mashberg A. Diagnosis of early mouth and pharyngeal squamous cancer: Obstacles and improvement. Oral Uncol. 2000; 36: 253-255.
13. Banoczy J, Ceba A. Occurred epithelial dysplasia in the oral cavity. Oral Sorg 1976; 42: 766-774.
14. Wright gm. Oral severe lesions and conditions. Simin Dermatol 1994; 13: 125-131.
15. Day of shame, stain Wei. Primary tumors are second in patients with oral cancer. Cancer 1992; 70: 14-9.
16. Schwartz L., Uzahin M, Chang Gun, et al. Synchronous and booming head and neck cancer. Cancer 1994; 74: 1933-8.
17. Gorski M, Silverman S Jr. The use of tobacco in patients with head and neck cancer: the second and second oral cancer / oral pharyngitis changes in patients from San Francisco. Cancer J 1994; 7: 78.
18. Grinspan, D. (1993). Enfermedades de la Boca. Tomo V. Editorial Mundi S.A.I.C.y F., ISBN:970-585-010-0, Buenos Aires Argentina.
19. Hindle, M., Downer, D., Moles D. & Speight P. (2004). Is alcohol responsible for more intraoral cancer? Oral Oncol Vol 34, pp. (328-333). ISSN: 1348-2375
20. Hinds E. (1971). Dental Care and Oral Hygiene Before and After Treatment. Radiation
21. Caries. J Am. Med Assoc, Vol 210, pp. (9064-6). ISSN: 1548-3595.
22. Humphris, G., Freeman R. & Clarke H. (2004). Risk perception of oral cancer in smokers attending primary care: a randomized controlled trial. Oral Oncol. Vol. 40, No. 9, pp. (916-929). ISSN: 1368-8375
23. Jansma, J., Vissink, A., Gravenmade, E., Visch L., 24.Fidler V. & Retief D. (1989). In vivo study on the prevention of post-radiation caries. Caries Res, Vol 69, pp. (175-174). ISSN:00084-6569
25. Jansma, J., Vissink, A. & Jongebloed, W., Retief, D., Johannes’s-Gravenmade, E. (1995). Natural and induced radiation caries: a SEM study. Am J Dent, No. 6, pp. 136–137. ISSN: 08945-8274
26. Jongebloed, W., Gravenmade, E. & Retief, D. (1988). Radiation caries. A review and SEM study. Am J Dent Vol. 2, pp. (134–145).ISSN: 0893-8274
27. Jovanovic, A., Kostense, P., Schulten, E., Snow G. & Van Der Waal, I. (1993). Delay in diagnosis of oral squamous cell carcinoma; a report from the Netherlands. Eur J Cancer B Oral Oncol, 28B, pp. (37–8). ISSN: 0964-1955
28. Jovanovic, A., Schulten, E. & Kostense, P. et al. (1993). Tobacco and alcohol related to the anatomical site of oral squamous cell carcinoma. J Oral Pathol Med, Vol 22, pp. (459-462). ISSN: 0904-2512
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Cancer"
Cancer is a disease in which cells grow or reproduce abnormally or uncontrollably. Cancerous cells have the potential to spread to other areas of the body in a process called metastasis.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: