Nutritional Status and Management of End-stage Renal Disease Patients Who Are Maintained on Chronic Dialysis
Info: 10270 words (41 pages) Dissertation
Published: 9th Dec 2019
Wasting in Chronic Kidney Disease
“Nutritional status and management of end-stage renal disease patients who are maintained on chronic dialysis”
Table of Contents
Table of contents……………………………………………………………………….… 2
Abstract………….…………………………………………………………………….……3
- Introduction……………………………………………………………………….….4-7
- Nutritional importance in chronic dialysis patients………………………….……..7
- Obesity………………………………………………………………………….……..7
- Protein-energy wasting……………………………………………………….……..8
1.4.1 Defining protein-energy wasting…………………………………….………8
1.4.2 Causes of protein-energy wasting……………………………….………….8
1.5 Aims and Objectives of thesis……………………………………………………..10
2 Literature review………………………………………………………..……………..11
2.1 Overview……………………………………..……………………….………………11
2.2 Kidney failure……………………………………………………………………………11
2.2.1 Urea……………………………………………………………………………11
2.2.2 Hypertension…………………………………………………………………..12
2.2.3 Diabetes……………………………………………………….……………12-13
2.3 Organisations………………………………………………………………………….13
2.4 Haemodialysis…………………………………………………………………….13-16
2.5 Peritoneal dialysis…………………………………………………………………16-18
2.6 Transplant…………………………………………………………………………..19-20
2.7 Potential treatments……………………………………………………………….20-21
3 Methodology…………………………………………………………………………….22
3.1 Overview…………………………………………….…………………………..…….22
3.2 Search strategy………………………………………………………………………22
3.3 Selection criteria………………………………………………………………………23
4 Discussion………………………………………………………………………………24
4.1 Major findings………………………………..……………………………………..24-25
4.2 limitations……………………………………………………………………………….25
5 Conclusion………………………………………………………………………………26
5.1 Overall conclusion…………………………………………………………………….26
5.2 Recommendation of future research…………………………………………………26
References………………………………………………………………………………27-29
Acknowledgments…………………………………………………………………………30
Abstract
Muscle wasting is the gradual deterioration of an individual typically due to a loss in strength and muscle mass often leading to conditions such as Chronic kidney disease. Chronic kidney disease (CKD) is a complex disease affecting millions of people around the world. The progression of CKD is associated with a number of complications through cardiovascular disease and diabetes. Through these conditions there is a gradual loss of function in kidneys and patients would need to be put onto dialysis treatment. Survival rates of patients undergoing dialysis are decreasing over the years and a need to find a steady treatment is of important paramount.
The objective of this thesis is, through a critical review of relevant literature aimed at finding the best possible treatment in which survival rates of patients keep at a moderate rate. Comparing different techniques of dialysis such as hemodialysis, peritoneal dialysis and also kidney transplant will be compared by a review of relevant literature from primary and secondary publications. Furthermore, other forms of treatments besides dialysis are discussed as potential treatments. The potential advantages of the treatment methods were central to choosing the best approach.
After full review, the study concluded that the best form of treatment for chronic kidney disease patients undergoing chronic dialysis is haemodialysis. As it is the best form of treatment in terms of its knowledge around it in comparison to peritoneal dialysis which needs further investment and training in order to fulfil its correct manner of treatment. However, the findings are limited by the scope and time of the review.
Keywords: Chronic kidney disease, Protein energy wasting, hemodialysis, peritoneal dialysis, kidney transplant
Chapter 1 – Introduction
1.1 Chronic kidney disease (CKD) is a major health problem affecting 10% of the population worldwide (Hallan et al; 2006). According to the Global Burden of Disease study, CKD is ranked 27th in the list of total deaths in 1990 worldwide, which further rose to 18th in 2010 (Jha V, 2013).This is further implied by the World Health Organisation (WHO), that in 2005 there were 58 million deaths worldwide and 35 million credited towards chronic diseases (Levey AS, 2007).Chronic conditions are identified by the WHO as being “health problems that require ongoing management over a period of years and decades” which is labelled as being one of the biggest challenges faced within the 21st century (GPM, 2014).
CKD is characterized by the failure of the kidneys to remove excess fluids and waste products from the body. There are different degrees of renal dysfunction from premature kidney damage to end-stage renal disease, in which have been classified into five stages on the basis of kidney damage and level of function (glomerular filtration rate) (National Kidney Foundation, 2002).
Some of the principal causes of CKD are hypertension, diabetes mellitus, glomerulonephritis and renal vascular disease. The risk of CKD increases with age but lifestyle factors do play a part in the progression of CKD. Obesity leads to CKD through hypertension and diabetes, but there has been emerging evidence that through obesity, there are other mechanisms involved such as inflammatory, metabolic and hemodynamic mechanisms (Iseki, 2004). Furthermore, an even more recent development in the pathophysiology of obesity-related kidney disease is that chronic inflammation and abnormal lipid metabolism contribute towards kidney cell damage. The study found that there is an increased risk of children with severe obesity to suffer from early stage kidney abnormalities, reduced kidney functions and elevated biomarkers of early kidney injury (Nehus, 2018). For patients in this situation, one of the ways in which the management of this is through bariatric surgery. Longitudinal studies in both adults and children that suffer from obesity-related kidney disease have improved kidney function after bariatric surgery (Nehus, 2018).
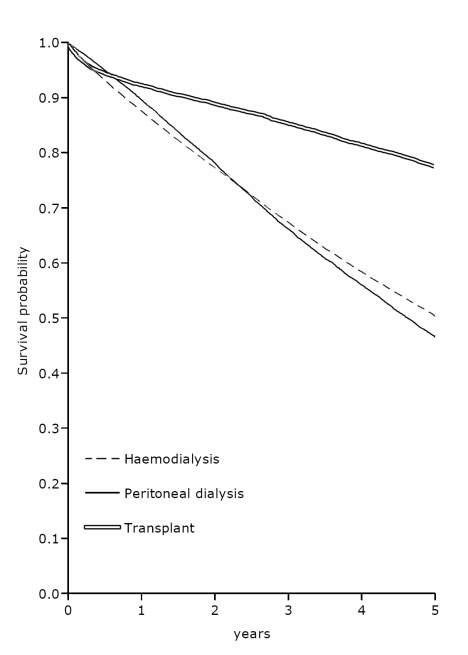
Figure 1. Survival of dialysis patients and patients receiving first transplant in Europe 1996-2000 (ERA-EDTA Registry 2005 Annual Report)
Patients who are in a more severe stage of chronic kidney disease are known to be at stage 5. Once this stage has been reached, renal replacement therapy becomes essential. However, a small percentage of people do reach end-stage renal disease, with estimates varying from 0.1 to 2.6 per 100 patients with stage 3 to 4 CKD (Hallan SI, 2006).
The mortality rates in figure 1 shows the various treatments used, in relation to the probability of survival in patients with CKD. It illustrates that patients who undergo kidney transplant have a better chance of survival. However, even though kidney transplant is the best option, not all people fulfil the criteria to undergo this treatment. Waiting lists to match kidney remain a constant problem as it does take a long time to match a donor. The renal replacement therapy (RRT) in figure 1 shows that it has had an effect on mortality rate but as years increased, the survival rates decreased.
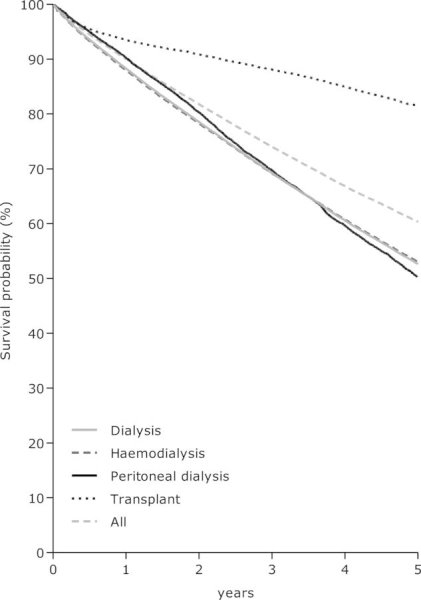
Figure 2. Survival of dialysis and renal transplant between 2002-2009 (Noordzij, 2011)
Dialysis has offered life-saving renal replacement therapy (RRP) for patients since the years 1960s (Scribner BH,1960).As years have gone by, techniques have developed to increase survival rates, but mortality remains stagnant. Figure 2 shows how one study presents the survival rates in comparison to figure 1. Transplant still remains higher in survival rates and the different forms of dialysis has lower survival rate (Noordzij, 2011).This shows how the management of CKD needs a more sophisticated treatment in increasing survival rates for patients with CKD.
1.2 The Importance of nutrition in Chronic Dialysis Patients
A patient’s nutritional status can have an adverse effect in the risk factors for mortality, when undergoing dialysis. The WHO defines malnutrition as deficiencies, excesses or imbalances in a person’s intake of energy and nutrients (World Health Organization. 2016). Both undernutrition and overnutrition are highly predominant within dialysis patients. The prevalence of undernutrition also defined as protein-energy wasting (PEW), ranges between 29% and 48% at the start of dialysis (Jansen MA, 2001).Once dialysis has started, the prevalence of PEW ranges from 23% to 76% in patients undergoing hemodialysis, and 18% to 50% in peritoneal dialysis patients (Jansen MA, 2001).This may suggest that hemodialysis may not be an ideal form of treatment in patients suffering from CKD. Around 10% of patients suffer from severe forms of PEW.Furthermore, the prevalence of obesity, which is expressed as BMI>30 kg/m2 is said to be around 30% at the start of dialysis (Jansen MA, 2001). Protein-energy wasting will be emphasised greatly within this thesis. The following paragraphs will describe the survival on obesity and the existing knowledge around PEW within dialysis population.
1.3 Obesity
Obesity has been recognised as a high-risk factor for increased mortality and morbidity within the general population. One study has proven the opposite that there is an increased survival rate with obesity. The study proved that with sufficient dialysis and special attention, normal BMI can be achieved and help reduce mortality and morbidity rates in patients undergoing hemodialysis (Fleischmann E, 1999).This in turn suggests that having a lower BMI increases mortality rate. This puts further emphasis on PEW being more of a key player in increased mortality rates on patients undergoing dialysis.
1.4 Protein-energy Wasting
1.4.1 Defining Protein-Energy Wasting
There are two main types of malnutrition in which have been described by a consequence of insufficient dietary intake with distinctive clinical symptoms: one of the symptoms is kwashiorkor due to a depletion of protein, and marasmus due to both depletion of protein and energy storage (Rao KS, 1974).When signs of both marasmus and kwashiorkor are present, often it has been referred to protein-energy malnutrition (Rao KS, 1974). In 2007, a professional board of the International Society of Renal Nutrition and Metabolism (ISRNM) suggested that the term ‘protein-energy wasting’ should be referred to the indication of the loss of body protein mass and fuel in CKD (Jansen MA, 2001).
1.4.2 Causes of Protein-Energy Wasting
Recent research has suggested that protein energy wasting (PEW) has other factors which contribute to the development of PEW, apart from insufficient food intake and reduced appetite, more so dietary restriction. Within protein-energy wasting some of the factors involved in the pathophysiology is an increase in energy expenditure, inflammation, anorexia and also insulin resistance (Mak, R., 2011). One study which supports the concept that there are multiple factors involved, goes by the notion that people who are suffering from muscle wasting have increased mortality and a decreased quality of life which is characterized by anorexia and degradation of muscle protein. This suggests that there are nutritional influences and nutritional imbalance in PEW (Siew, E. and Ikizler, T. 2010).
Pre-dialysis patients are normally advised to reduce their protein intake in order to reduce uremic symptoms in which this slows down the progression of renal failure (Kopple JD ,2000). Furthermore, when patients are maintained on dialysis, inadequate dietary factors increase the nutritional requirements.During dialysis energy expenditure is increased, therefore, increasing the energy requirements (Kopple JD, 2000).
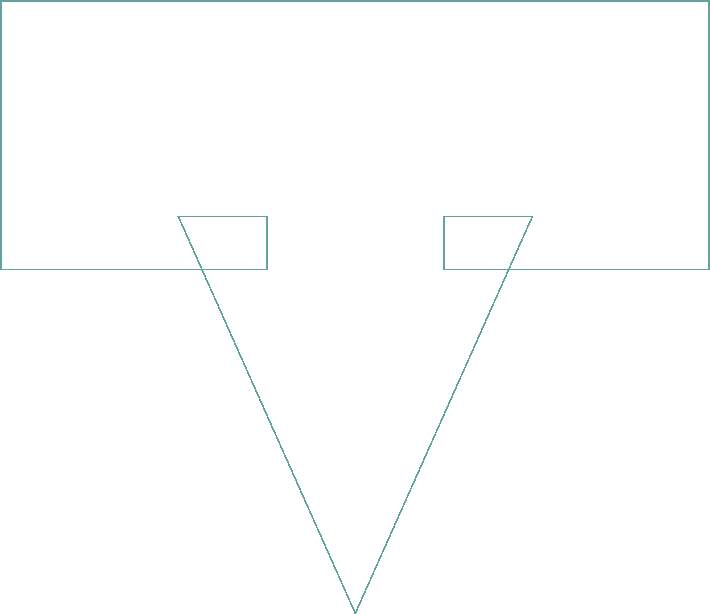
Decreased nutritional intake
- Loss of renal function
- Dietary protein restriction
- Decreased appetite
- Anorexia
- Nausea, Vomiting
Increased nutritional requirements
- Chronic kidney disease:
Impaired IGF-1, metabolic acidosis, impaired protein assimilation, endocrine abnormalities
- Comorbid conditions:
Diabetes mellitus, Atherosclerotic cardiovascular disease, heart failure, impaired endothelial function
- Inflammation:
Inflammatory cytokines, infections
- Dialysis treatment associated factors:
Nutrient loss via dialysis, arteriovenous graft
Protein-energy wasting


Quality of life
Hospitalisation
Mortality
 Figure 3: Schematic representation of the possible causes and consequences of PEW in CKD.
Figure 3: Schematic representation of the possible causes and consequences of PEW in CKD.
1.5 Aim(s) and Objectives of thesis
The aim of this thesis is to critically evaluate wasting in chronic kidney disease through the use of primary and secondary literature sources and look at how this impacts on survival rates on patients undergoing chronic renal dialysis.
The main objective of this thesis, is to find the best possible form of treatment in end-stage renal disease patients who are maintained on chronic dialysis treatment. To put this in perspective, when comparing the survival rates of figure 1 and 2 in dialysis and transplant, it shows how far we have come in finding the correct management in patients undergoing dialysis. Therefore, this thesis also aims to further the understanding of the best possible treatment available in increasing survival rates for dialysis patients.
Chapter 2 – Literature Review
2.1 Overview
In this chapter, a detailed account of the cause of renal failure will be analysed in depth and relevant literature relating to my research will be critically analysed through primary and secondary publications, alongside other significant publications will be reviewed. All accounts of specialist organisations will be given. Through this analysis, a means of finding the best possible form of treatment will be addressed.
2.2 Kidney failure
Chronic kidney disease is a broad term that includes subtle decrease in kidney function, that develop over a minimum of three months. In contrast, acute kidney disease refers to any deterioration in kidney function that occurs less than three months.
Blood enters the kidney through the renal artery and once it is inside, it enters arterioles called glomeruli, where initially filtration occurs. The filtrate moves into the renal tubule. The rate at which filtration takes places is known as glomerular filtration. In a normal healthy person, this is between 100-120 millilitres of filtration per minute per 1.73m2 of body surface area. This value is slightly less in women than men, but decreases further with age (Levey et al., 2003).
2.2.1 Urea
Urea normally gets excreted in the urine, but when there is a decrease in the glomerular filtration rate, less urea gets filtered out. Therefore, it builds up within the blood which leads to a condition called azotemia. Azotemia can cause symptoms such as nausea and loss of appetite. As urea levels increase, it can have an effect on the central nervous system causing encephalopathy. This results in asterixis which is a tremor of the hand which resembles a bird flapping its wings and is best seen when a person attempts to extend their wrists (The National Kidney Foundation, 2017).
Further accumulation of urea can even lead to coma or even death. Even further increase can lead to a condition called pericarditis which is inflammation of the lining of the heart. In addition, there is an increase tendency of bleeding, since excess urea in the blood makes platelets less sticky leading to less clot formation. In some cases, an individual can develop a condition called uremic frost where urea crystals can deposit within the skin (The National Kidney Foundation, 2017).
Key hormones are released by the kidney. When the kidney senses a lower than normal amount of fluid getting filtered, it responds by releasing a hormone called renin to increase blood pressure. In chronic kidney disease, the decrease in glomerular filtration rate leads to an increase in renin secretion leading to hypertension.
2.2.2 Hypertension
One of the most common cause of CKD is hypertension. In hypertension, the walls of the arteries supplying the kidney begin to thicken in order to withstand the pressure, which results in the narrowing of the lumen. This leads to a decrease in blood and oxygen to the kidney, resulting in ischemic injury to the nephrons glomerulus.
Immune cells like macrophages and fat-laden macrophages called foam cells enter the damaged glomerulus’s and begin to secrete growth factors, such as transforming growth factor 1. These growth factors cause the mesangial cells to regress back to their more immature stem state known as mesangioblasts and secrete extracellular structural matrix. This extracellular matrix leads to glomerulosclerosis which is hardening and scaring. This reduces the nephrons ability to filter blood and over time leading to CKD (Tedla et al., 2011).
2.2.3 Diabetes
The second most common cause of CKD is diabetes. Excessive glucose in the blood start sticking to proteins within the blood, through a process called non-enzymatic glycation due to no enzymes being involved. The process of glycation particularly affects the efferent arteriole, which causes it to become stiffened and narrowed. This in turn creates an obstruction that makes it difficult for blood to leave the glomerulus and increases pressure within the glomerulus leading to hyperfiltration (Levey et al., 2003).
In response to this high-pressure state, the supportive mesangial cells secrete structural matrix which expands the size of the glomerulus. The process of glomerulosclerosis also reduces the nephrons ability to filter blood leading to chronic kidney disease.
2.3 Organisations
Several specialist organisations study, monitor and develop strategies for management and treatment of renal conditions. They include; National Institutes of Health, National Institute of Diabetes and Digestive Kidney Diseases, Division of Kidney, Urologic and Haematological Diseases. But the largest and most wide spread is The United State Renal Data System (USRDS), which was established in 1989 national end-stage renal disease (ESRD) and chronic kidney disease surveillance organisation (US Renal Data System, 2007). It has been operating for 25 years alongside its competitors. Within its first 10 years, it has developed strategies in which calculating prevalence and incidence of treated ESRD and also reported its mortality outcomes in both dialysis and renal transplant populations. Its focus changed within its third and fourth contract period towards the calculation of cause-specific morbidity and mortality. It therefore expanded its domain of care beyond dialysis therapy delivery (US Renal Data System, 2007). This further indicates the need of a more improved strategy in maintaining survival rates of patients undergoing dialysis.
2.4 Haemodialysis
Hemodialysis is a treatment of purifying the blood through a dialysis machine, in which is done several times a week. The blood therefore is filtered outside of the body. Unfiltered blood is removed from the body and flows through a dialyzer to be purified. Filtered blood then flows back into the body.
Patients who undergo dialysis are thought to have a low health-related quality of life (HRQOL). This in turn increases the risk of a patient’s mortality and hospitalization. A recent study done by (Broers et al., 2018) aimed to look at patients who are on stage 5 CKD, and compared HRQOL. The test was run within the first year of patient dialysis. The method used in this study constituted of short term questionnaires to measure mental and physical areas of health with scores. It scored using physical component summary (PCS) and mental component summary (MCS). The study concluded that a patients HRQOL is already low when at stage 5 of CKD and within the first year of dialysis, there is no significant change in the quality of life. However, the study also concluded that physical activity in relation to the PCS score, physical activity may be a potential tool to improve HRQOL in patients on stage 5 CKD. This in turn goes to show that along with this type of dialysis, a patient’s quality of life will only improve with a correlation of physical activity.
The study strongly suggests that this form of dialysis may not be the best option as it requires physical activity when patients are already on stage 5 CKD. Patients may not be able to perform basic physical activities during stage 5 CKD in which shows that this study proves that this form of dialysis may not improve mortality rates. However, this study based its results on treatment after only one year. Patients HRQOL may improve after three years of dialysis or physical activity alongside dialysis may cause a patient’s condition to deteriorate further in the long term. Therefore, this study still remains questionable to whether physical activity improves mortality rates alongside dialysis treatment.
With hemodialysis, it involves a catheter being introduced into the patient’s blood stream. With that comes along infections which can be caused by the catheter. A study done by (Yap et al., 2018) looked at patients undergoing hemodialysis in Singapore. It examined catheter-related blood stream infections. It ran a single-centre retrospective analysis of patients on hemodialysis between January 2010 and December 2012. The results showed that initiation of dialysis via a catheter is strongly associated with an increase in mortality rates. In particular, with the presence of diabetes and catheter-related bloodstream infection, the mortality is increased further. A more interesting result found within this study showed that there was a decrease in mortality rates in patients who were seen by a nephrologist before starting dialysis.
This study done by (Yap et al., 2018) concluded that prolonged duration of catheter is found to be a risk factor of increasing infection. This in turn suggests further that haemodialysis may not be a sufficient treatment in order to maintain stability with mortality rates of patients. However, the study was carried out in Singapore, a country in South East Asia where the environment may have more infections present when comparing UK or the USA. This may contribute as a factor in mortality rates, where the patient’s environment is completely free from foreign pathogens.
A more wider approach by (Ravani et al., 2017) looked at similar associations of hemodialysis and morality. The study was done on patients who started hemodialysis from Europe, North America and Australasia. The study evaluated associations between access type and time to infectious and non-infectious complications. The results of the study showed that out of 6119 adults around 2084 patients developed a non-infectious complication and 542 developed an infectious complication. This in turn shows that other than infections, there may be other factors which contribute to the increase in mortality in patients undergoing haemodialysis.
During haemodialysis, the prevalence of severe vomiting and nausea are present. A study done by (Asgari et al., 2016) looked at the incidence of vomiting and nausea of patients undergoing haemodialysis. The objective of the study was to determine the incidence of vomiting and nausea in a group of patients. The way the study was carried out was by verbal numeric rating scale (VRNRS) and korttila vomiting scale. These were used to measure the severity of nausea and vomiting during haemodialysis. The results of the study showed the incidence of vomiting and nausea were respectively 28.3% and 11.7%. Furthermore, the mean severity of nausea was 1.15 and 2.08 for vomiting. The study concluded showing a high incidence rate of both vomiting and nausea and certain measures have to be taken by nurses in order to help prevent the occurrence of vomiting and nausea.
This study highlights the major problem with haemodialysis and vomiting itself. During vomiting essential electrolytes are lost, in contrast to chronic kidney disease where essential nutritional elements are already decreased. This makes vomiting during dialysis a dangerous form of treatment. But the most important point from the study is within the introduction as it highlighted, the great progress with haemodialysis equipment but is associated with many complications. This in turn strongly suggests that haemodialysis is not a suitable treatment for patients in ESRD. This is further supported by (Igarashi et al., 2013) who emphasises nausea and vomiting in a patient undergoing chronic dialysis.
Overall, haemodialysis is proved to be a treatment that causes mortality rates to increase rather than improve mortality. In particular, the presence of infection is high and occurs frequently during dialysis. (Collins et al., 2009) examined trends within ESRD programs, assessing progress in preventative care, hospitalization and mortality since 1989. The number of patients undergoing dialysis has almost tripled to 336,00 in 2007 from 123,00 in 1989. The most important factor mentioned by (Collins et al., 2009) is that for incident patients, infectious hospitalization increased to almost 100% over the last 10 years. Furthermore, the use of catheters is around 82% which shows the use of it is high. Poor planning for dialysis may contribute to the use of catheter in which may contribute to the high association of infection which limits the potential patient survival.
In relation to the study done by (Yap et al., 2018), mortality rates are lower when a patient is seen by a nephrologist before initiating dialysis. This shows there may be a lack of experienced hospital staff contributing towards mortality rates of patients undergoing going haemodialysis. This further puts into perspective whether haemodialysis is a safe treatment in the long term.
2.5 Peritoneal dialysis
Peritoneal dialysis uses the lining of the abdomen or stomach, which filters blood inside the body. There are two types of peritoneal dialysis; Continuous ambulatory dialysis (CAPD) which is done manually and automated peritoneal dialysis (APD) which uses a cycler machine when patient is sleeping.
During peritoneal dialysis, fluid is drained into the peritoneal cavity, allowed to sit here for several hours whilst it absorbs waste products and then drained out. The process is repeated several times a day and can effectively replace kidney function, as it is a continuous process which allows the patient to carry out with normal activities (CAPD). In a study done by (Sakacı et al., 2015), the clinical outcomes were evaluated and identified for mortality within elderly patients undergoing peritoneal dialysis, in particular peritoneal dialysis. The results of the study showed that during follow up periods, some patients were withdrawn due to death. The main causes of death included sepsis and peritonitis (50%) and cardiovascular events (30%). It concluded that mortality is higher within elderly patients and factors effecting mortality included advanced age, presence of comorbid diseases and interestingly continuous ambulatory dialysis.
Likewise, with haemodialysis, infections are also prevalent within peritoneal dialysis which advocates it may also be a treatment which is not effective and causes mortality rates to increase. However, the study took into account only elderly patients over 65. With age, the immune function reduces which make infections more prone towards elderly. This may be a factor contributing to the increase in mortality rates. Furthermore, with CAPD, it can be performed by one’s self, which may cause elderly to perform techniques incorrectly causing further infection. This suggests CAPD may not be an effective form of treatment in keeping mortality stable.
Similarly (El-Reshaid et al., 2016) ran a study to evaluate patient survival in both CAPD and APD. The retrospective study took into account infection rates, in particular peritonitis which is a common infection present in dialysis. 180 patients on CAPD and 128 patients on APD were compared in the period between January 2004 and December 2014. The ten-year study showed significant conclusions as patients on APD had a lower incidence rate of peritonitis infection which lead to a decrease in mortality rates.
The fact that APD had a significant result in decreasing mortality rates shows that technology may have a factor in increasing or decreasing patient survival in dialysis. It may be the case that for both techniques of dialysis (haemodialysis and peritoneal) it would have significant result on mortality if man made automation could be out into effect. This may further decrease infection rates and increase survival of patient.
This is further emphasized by (Chen et al., 2018) in a scientific report that technique failure is a frequent obstacle of peritoneal dialysis. He examined this by Using Australian and New Zealand Dialysis and Transplant (ANZDATA) registry data, and examined the associations between technique failure, causes and mortality in all incident PD patients who experienced technique failure between 1989-2014. Factors such as social reasons and age were taken into account which may have an effect on mortality. This recent study highlights further that dialysis is not an applicable form of treatment but may need technology aid in preventing infection and causing mortality to decrease.
In contrast, peritoneal dialysis has thought to have better patient outcome in comparison to haemodialysis. A study carried out by (Li et al., 2016) put great emphasis on the increased utilization of peritoneal dialysis in countries such as the USA, China and Thailand, but a decrease in peritoneal dialysis in most European countries and in Japan. The most important factor highlighted is the fact that there are key strategies in the process of peritoneal dialysis in regard to the implementation and procedure, in order for the peritoneal dialysis fluid to be supplied at a low cost. Furthermore, the emphasis on training being provided to nurses is of high paramount. The study concluded by underlining the importance in training in order for peritoneal dialysis being a more efficient form of treatment. Also, highly stressing on the factor of more investment being needed towards research and training. This suggests that peritoneal dialysis may potentially become a more worldwide form of treatment but when looking at the economic side of it, it may be costly.
However, in an earlier study by (Lameire and Van Biesen, 2009) an estimated 1.77 million patients received dialysis worldwide and of these patients 1.58 million received haemodialysis. It was further estimated that 190,000 of these patients received peritoneal dialysis. Similarly, the important factor in the higher use of hemodialysis was due to mainly economic and educational factors and the study also mentions, in order to reverse the trends, the implementation of strategies in peritoneal dialysis is needed. Also increasing investment into more training for peritoneal dialysis is needed.
When comparing both studies it suggests that there may be potential in the treatment of peritoneal dialysis. The high emphasis on further investment and education towards peritoneal dialysis in both studies, could mean that haemodialysis is losing its value in terms of patient satisfaction and survival and a more adverse form of treatment is needed to increase the survival rates of patients undergoing dialysis.
2.6 Transplant
In more serious life-threatening cases, kidney transplants are performed in order to replace the non-functional kidney. However, various problems occur during transplant such as rejection of recipient cells and finding a suitable kidney donor. Financially, transplants are costly throughout health sectors. The most common problem with transplants is patient waiting list and this may have an effect on the already deteriorating health of a CKD patient.
This is highlighted by (Reese et al., 2015) who ran a study based on the global health of patients awaiting kidney transplant and identifying which patients will derive a survival benefit from getting transplant in comparison to receiving dialysis. The fundamental conclusion of the study was that even patients who have a low function appear to live longer with having a kidney transplant comparing to receiving dialysis. Further emphasized that waiting listed patients, global health measures like functional status may be more useful in counselling patients about the probability of transplantation than in identifying who will derive a survival benefit from it.
A study done by (Cheddani et al., 2018) focused on kidney transplant patients. Its main focus was to evaluate aortic stiffness by carotid-femoral pulse wave velocity (CF PWV). This was a predictor of mortality within several populations. The method by which the investigation was carried out was that it based a retrospective cohort study of 220 kidney recipients, three months after transplantation. Within the study the two primary end points were the cause of mortality and occurrence of end stage renal disease at the start of dialysis. After a follow up of 5 years, death occurred in 10 -12 patients respectively. More so, the CF-PWV was a neutral mortality risk factor. It concluded that aortic stiffness that is measured three months after kidney transplant is a strong indicator of mortality.
Transplants may have lifesaving effects but one of the major problems of post transplants are hypercalcemia. In turn, this has an effect of the patient’s survival. A study by (Demir et al., 2018) talked about a 66 years old kidney transplant recipient who was admitted to hospital due to symptoms of fever, vomiting and nausea. The laboratory results showed normal kidney function but high levels of serum calcium. The patient was treated by various types of medication such as isotonic saline with furosemide but were not effective. Then haemodialysis was applied along with low calcium dialysate for three successive days in which resulted in normal levels of calcium. Despite treatment, the patient later died of septic shock but the important aspect to highlight here is the fact that haemodialysis was needed even after transplant in which the patient’s life was prolonged. If haemodialysis was not given the patient would have died earlier. This strongly suggests that transplant may not be a suitable form of treatment in end stage renal patients.
2.7 Potential Treatments
As mentioned before, PEW is caused by factors such as inflammation and insulin resistance. One study puts emphasis on insulin resistance and protein energy metabolism. Within the overall population, insulin resistance has been linked to accelerated protein catabolism (Siew, E. and Ikizler, T. 2010). Amid ESRD patients, this break down of protein has been observed for patients with type 2 diabetes in comparison to ESRD patients without diabetes. In the absence of diabetes, insulin is detectable more strongly and has an increased muscle protein breakdown. The study indicates further, that recent epidemiological data has shown an advantage in survival and better nutritional status in insulin free type 2 patients who are treated with insulin sensitizer thiazolidinedione (Siew, E. and Ikizler, T, 2010). This proved to be an important outcome and could represent a new intervention for ESRD patients.
However, a more recent study was carried out on insulin sensitivity in non-diabetic end-stage renal subjects who are maintained on dialysis. These subjects took a drug named pioglitazone with belongs to a class of drugs known as thiazolidinedione, similar to the study above. The results of the study showed an improvement in hepatic insulin sensitivity and a reduction in cardio-metabolic markers. In regard to whether or not the effect improved the outcome of non-diabetic ESRD still needs further evaluation (Zanchi, A, 2014).
These studies show that insulin therapy is not a good management technique, even though the first study showed some important advances, it only accounted for patients without diabetes and not with type 2 diabetes. This in turn doesn’t account for the general population, which makes it an unsuitable technique and has an effect on the overall survival rate.
This may further be due to a study which looked at the insulin growth factor (IGF-1). It looked at the correlation between PEW and IGF-1 and whether or not if any disturbances in the growth hormone in ESRD has any influences on the impact of survival in PEW. Subjects were categorized according to the levels of IGF-1 at the start of dialysis. The results showed that a low level of IGF-1 has an increased risk of mortality, more so inefficiency in IGF-1 contributes to PEW in ESRD. This could postulate that there is a connection between insulin therapy and a disturbance of the IGF-1 growth factor, which leads to a decrease in survival rates (Nilsson E, 2015).
With regards to inflammation, there have been substantial advances in that inflammation plays a key role within protein-energy wasting in patients who are undergoing kidney dialysis. One study looked at the interrelationship between PEW and inflammation on patients undergoing peritoneal dialysis. Patients were assessed with regards to their nutritional status and inflammation after a period of 3 months. The study concluded that PEW and inflammation are prevalent among patients undergoing peritoneal dialysis. More so, inflammatory markers show significant correlation and has been suggested to be used on a regular basis in the assessment of dialysis patients. Furthermore, for better management of PEW (Krishnamoorthy V, 2015).
In relation to inflammatory markers, a more recent study looked at the dietary inflammatory index (DII) in protein energy wasting in hemodialysis patients. The DII is a new tool for assessing inflammatory potential in the diet. The results showed significant correlation with consistent inflammation indicators. The study concluded that the DII tool is a positive way in assessing inflammatory potential when looking at dialysis patients (Kizil M, 2016).
Chapter 3 – Methodology
3.1 Overview
This section outlines the search strategy and selection criteria adopted for this review, and provides descriptions of the types of studies reviewed. Also contains the reason behind certain type of studies being considered within this review.
3.2 Search strategy
Relevant research concerning survival rates with the various forms of dialysis, other forms of treatment and transplant were identified by searching the most common search tool; PubMed. A number of different studies including cohort studies, longitudinal studies, meta-analysis, systemic studies, cross sectional studies and scientific articles were found. Ranging from the years 1984-2016. Basic google searches were made in order to obtain relevant facts and figures of chronic kidney disease.
In order to ensure relevant studies were not missed, the search terms remained broad and direct. These were “mortality or survival”, plus “dialysis” “chronic kidney disease” anywhere within the title or abstract. Studies were eligible for consideration within this review if: (a) the focus of the study was on chronic kidney disease and its management; and (b) there was at least a form of treatment and information on survival rates of patients suffering CKD.
Finally, a comprehensive search was also used from internet resources within the UK and abroad. A number of sites were used such as The World Health Organisation, national kidney foundation and NHS in order to obtain various information. Information relating to how different dialysis work and how they are different from each other. Furthermore, the techniques used for dialysis. Also exploring potential forms of treatments other than dialysis such as medication use.
3.3 Selection criteria
The next step in selecting relevant studies were excluding measures where chronic kidney disease, its treatments and survival rates were insufficiently described or whether further research was needed within the study, and therefore did not contribute to the important information within this review. For the studies investigating direct associations between mortality rates and CKD, the review included longitudinal studies. Longitudinal studies were seen as particularly valuable as they involve collection of data over a period of time, which can determine patterns competently. More so it allowed me to determine cause and effect relationships and make connection clearer.
Longitudinal studies were seen as a particularly valuable resource as they facilitate the testing of relationships between early events or characteristics and later outcomes, and enable the identification of developmental sequences and pathways, as well as the construction of theoretical models which can then in the future be validated. Cross-sectional studies which used large samples and methodologically sound research designs were also of benefit.
Studies which included test patients undergoing haemodialysis were of great benefit as it allowed me to gather important information regarding cause and effect relationship. Furthermore, it also provided me with information in which certain studies which still need further research. This in turn helped me identify gaps in terms of my research in which was selected to highlighting further research is needed.
Studies which contained cross sectional studies were considered as valuable information as it was of great benefit. This allowed me to look at larger populations and identifying key elements within survival rates in CKD patients undergoing dialysis. It further allowed for quick and easy gathering of information for a larger target population.
Chapter 4 – Discussion
4.1 Major findings
The best form of treatment in patients suffering end stage renal disease is haemodialysis. Haemodialysis is the best form as it provides the easiest and efficient way in treating patient suffering from end stage renal disease. After reviewing and researching different forms of treatment for chronic kidney disease such as peritoneal dialysis, transplants and other forms of treatments, the one which is most suitable in terms of keeping patient survival rates at a steady rate is through haemodialysis.
The main reason in coming to a conclusive finding of haemodialysis being the best form of treatment comes from the many complications associated with the other forms of treatment, such as peritoneal dialysis which further research and education are being needed to advance in that form of treatment. Furthermore, from reviewing the studies the most important reason in coming to a conclusion that haemodialysis is the best form of treatment is that for decades, this form of treatment has been the primary treatment for patients with end stage renal disease. However, (Abecassis, M., 2008) mentions in a study that the prime therapy for end stage renal disease is kidney transplantation. But from the study done by (Demir et al., 2018) highlights the major problem with transplantation.
As mentioned that the major problem with transplantation is hypercalcemia. The study highlighted that other forms of treatment were used to regulate and keep calcium levels stable, such as medication. But the factor which helped the patient’s calcium levels was the use of haemodialysis over a period of three consecutive days. The use of haemodialysis most probably kept the patient alive for longer. This goes to show that after all considerations, haemodialysis may be the last resort but has helped in saving and prolonging a patient’s life.
Taking into perspective the economic side of treatments such as more money being needed to invest in peritoneal dialysis shows that the other forms of treatment are not at best being used worldwide. Due to financial reasons, some countries may be using haemodialysis due to it being more cost effective. This is highlighted in the study by (Li et al., 2016) that the economic power houses such has the USA and china are investing money in more peritoneal dialysis. However, despite money being invested into peritoneal dialysis, the need for special training in delivering peritoneal dialysis is still in question. Furthermore, nurses need to be more educated in terms of the procedure of peritoneal dialysis. This puts heavy emphasis on the whole perception of the management of dialysis itself. Dialysis of a patient being either haemodialysis or peritoneal dialysis, the management of the two treatments may need to be further considered as both serve the same purpose but due to financial reasons only one is being considered highly than the other.
Transplants may be a more sufficient way in treating patient’s but as the study done by (Demir et al., 2018) shows the major problem with kidney transplant. Transplants possess more problems in terms of matching with the correct donor which is also time consuming since certain patients would need a transplant imminently in order to save their life. With transplants, there are high risks of rejection, which further makes it a treatment not as suitable.
In terms of potential treatments, the study by (Zanchi, A, 2014) shows possible advances in the use of medication but the treatment only took into account non-diabetic patients. As diabetic patients are more at risk of death there would need to be a more sufficient approach to other forms of treatment in order to maintain patient mortality.
4.2 Limitations
Throughout the review, my research has opened up potential flaws within certain studies. For example, majority of the studies have not included data regarding gender specificity. Whether it be male or female, studies have not clearly shown the extent of whether men or women would benefit from a certain type of treatment. One form of treatment may be more efficient in women than men. In that sense if peritoneal dialysis is more effective in men, then it would be beneficial to treat only men suffering from CKD to undergo peritoneal dialysis and women by means of haemodialysis.
Furthermore, diabetes is more prevalent within CKD and studies have shown that non-diabetic patients have more of a chance in survival during treatment in comparison to diabetic.
5 – Conclusion
5.1 Overall Conclusion
In conclusion to my review, takin in account all forms of treatments, the best form of treatment in terms of patient delivery, procedure, satisfaction and survival is haemodialysis. Also, due to the extensive knowledge around haemodialysis it forms the ideal treatment in end stage renal disease patients.
The aim and objective of the review were met as the best form of treatment is haemodialysis. However, the research can be improved further due to the limited time and scope of the research.
5.2 Recommendation of future research
Throughout my research, other than finding the best possible form of treatment for CKD patients, certain factors may have huge influences on certain studies. For example, one future research would be into technique failure in health professionals. Due to a lack of knowledge and experience, health professionals such as nurses who are newly qualified dealing with dialysis patients may contribute to mortality rates. Hence a future research would need to be carried out to investigate knowledge around the different forms of dialysis.
References
- Abecassis, M., Bartlett, S.T., Collins, A.J., Davis, C.L., Delmonico, F.L., Friedewald, J.J., Hays, R., Howard, A., Jones, E., Leichtman, A.B. and Merion, R.M., 2008. Kidney transplantation as primary therapy for end-stage renal disease: a National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQI™) conference. Clinical Journal of the American Society of Nephrology, 3(2), pp.471-480.
- Asgari, M., Asghari, F., Ghods, A., Ghorbani, R., Hoshmand Motlagh, N. and Rahaei, F. (2016). Incidence and severity of nausea and vomiting in a group of maintenance hemodialysis patients. Journal of Renal Injury Prevention, 6(1), pp.49-55.
- Broers, N., Martens, R., Canaud, B., Cornelis, T., Dejagere, T., Diederen, N., Hermans, M., Konings, C., Stifft, F., Wirtz, J., Leunissen, K., van der Sande, F. and Kooman, J. (2018). Health-related quality of life in end-stage renal disease patients: the effects of starting dialysis in the first year after the transition period. International Urology and Nephrology.
- Cheddani, L., Radulescu, C., Chaignon, M., Karras, A., Neuzillet, Y., Duong, J., Tabibzadeh, N., Letavernier, E., Delahousse, M. and Haymann, J. (2018). From arterial stiffness to kidney graft microvasculature: Mortality and graft survival within a cohort of 220 kidney transplant recipients. PLOS ONE, 13(5), p.e0195928.
- Chen, J., Johnson, D., Hawley, C., Boudville, N. and Lim, W. (2018). Association between causes of peritoneal dialysis technique failure and all-cause mortality. Scientific Reports, 8(1).
- Collins, A., Foley, R., Gilbertson, D. and Chen, S. (2009). The State of Chronic Kidney Disease, ESRD, and Morbidity and Mortality in the First Year of Dialysis. Clinical Journal of the American Society of Nephrology, 4(Supplement 1), pp.S5-S11.
- Demir, E., Karaoglan, C., Yegen, G., Sair, B., Yazici, H., Turkmen, A. and Sever, M. (2018). Extreme hypercalcemia in a kidney transplant recipient. CEN Case Reports.
- El-Reshaid, W., Al-disawy, H., Nassef, H. and Alhelaly, U. (2016). Comparison of peritonitis rates and patient survival in automated and continuous ambulatory peritoneal dialysis: a 10-year single center experience. Renal Failure, 38(8), pp.1187-1192.
- ERA-EDTA Registry: ERA-EDTA Registry 2005 Annual Report. Academic Medical Center, Department of Medical Informatics, Amsterdam, The Netherlands, 2007
- Fleischmann E, Teal N, Dudley J, May W, Bower JD, Salahudeen AK: Influence of excess weight on mortality and hospital stay in 1346 hemodialysis patients. Kidney Int 55:1560-1567, 1999
- GPM. (2014). Chronic Disease Management: The Pharmacist’s Role | GPM. [online] Available at: https://groupepremiermedical.ca/en/2014/03/20/chronic-disease-management-the-pharmacists-role/ [Accessed 11 Feb. 2018].
- Hallan SI, Coresh J, Astor BC, et al.: International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol 17:2275-2284, 2006
- Igarashi, Y., Akimoto, T., Nukui, A., Nakamura, H., Kawai, A., Kijima, S., Kubo, T., Sugimoto, H., Morita, T. and Kusano, E. (2013). Flank Pain, Nausea, Vomiting and Hypotension in a Chronic Hemodialysis Patient with a Spontaneous Perirenal Hemorrhage. Internal Medicine, 52(18), pp.2083-2086.
- Iseki K, Ikemiya Y, Kinjo K, Inoue T, Iseki C, Takishita S: Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int 65:1870- 1876, 2004
- Jansen MA, Korevaar JC, Dekker FW, Jager KJ, Boeschoten EW, Krediet RT: Renal function and nutritional status at the start of chronic dialysis treatment. J Am Soc Nephrol 12:157-163, 2001
- Jansen MA, Korevaar JC, Dekker FW, Jager KJ, Boeschoten EW, Krediet RT: Renal function and nutritional status at the start of chronic dialysis treatment. J Am Soc Nephrol 12:157-163, 2001
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. Jul 20 2013;382(9888):260-272.
- Kizil, M., Tengilimoglu-Metin, M., Gumus, D., Sevim, S., Turkoglu, İ. and Mandiroglu, F. (2016). Dietary inflammatory index is associated with serum C-reactive protein and protein energy wasting in hemodialysis patients: A cross-sectional study. Nutrition Research and Practice, 10(4), p.404.
- Kopple JD: The National Kidney Foundation K/DOQI clinical practice guidelines for dietary protein intake for chronic dialysis patients. Am J Kidney Dis 38:68-73, 2000
- Krishnamoorthy, V., Sunder, S., Mahapatra, H., Verma, H., Sharma, N., Jayaraman, R., Sathi, S., Khanna, S. and Mohamed, A. (2015). Evaluation of Protein-Energy Wasting and Inflammation on Patients Undergoing Continuous Ambulatory Peritoneal Dialysis and its Correlations. Nephro-Urology Monthly, 7(6).
- Lameire, N. and Van Biesen, W. (2009). Epidemiology of peritoneal dialysis: a story of believers and nonbelievers. Nature Reviews Nephrology, 6(2), pp.75-82.
- Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: approaches and initiatives – a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. Aug 2007;72(3):247-259.
- Levey, A., Coresh, J., Balk, E., Kausz, A., Levin, A., Steffes, M., Hogg, R., Perrone, R., Lau, J. and Eknoyan, G. (2003). National Kidney Foundation Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Annals of Internal Medicine, 139(2), p.137.
- Li, P., Chow, K., Van de Luijtgaarden, M., Johnson, D., Jager, K., Mehrotra, R., Naicker, S., Pecoits-Filho, R., Yu, X. and Lameire, N. (2016). Changes in the worldwide epidemiology of peritoneal dialysis. Nature Reviews Nephrology, 13(2), pp.90-103
- Mak, R., Ikizler, A., Kovesdy, C., Raj, D., Stenvinkel, P. and Kalantar-Zadeh, K. (2011). Wasting in chronic kidney disease. Journal of Cachexia, Sarcopenia and Muscle, 2(1), pp.9-25.
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification and Stratification. Am J Kidney Dis 39(suppl 1):S1- S000, 2002
- Nehus, E. (2018). Obesity and chronic kidney disease. Current Opinion in Pediatrics, p.1.
- Nilsson, E., Carrero, J., Heimbürger, O., Hellberg, O., Lindholm, B. and Stenvinkel, P. (2015). A cohort study of insulin-like growth factor 1 and mortality in haemodialysis patients. Clinical Kidney Journal, 9(1), pp.148-152
- Noordzij, M.Kramer, Renal replacement therapy in Europe: a summary of the 2011 ERA-EDTA Registry Annual Report. Clinical Kidney Journal, 7(2), pp.227-238.
- Rao KS: Evolution of kwashiorkor and marasmus. Lancet 1:709-711, 1974
- Ravani, P., Quinn, R., Oliver, M., Robinson, B., Pisoni, R., Pannu, N., MacRae, J., Manns, B., Hemmelgarn, B., James, M., Tonelli, M. and Gillespie, B. (2017). Examining the Association between Hemodialysis Access Type and Mortality: The Role of Access Complications. Clinical Journal of the American Society of Nephrology, 12(6), pp.955-964.
- Reese, P., Shults, J., Bloom, R., Mussell, A., Harhay, M., Abt, P., Levine, M., Johansen, K., Karlawish, J. and Feldman, H. (2015). Functional Status, Time to Transplantation, and Survival Benefit of Kidney Transplantation Among Wait-Listed Candidates. American Journal of Kidney Diseases, 66(5), pp.837-845.
- Sakacı, T., Ahbap, E., Koc, Y., Basturk, T., Ucar, Z., Sınangıl, A., Sevınc, M., Kara, E., Akgol, C., Kayalar, A., Caglayan, F., Sahutoglu, T. and Ünsal, A. (2015). Clinical outcomes and mortality in elderly peritoneal dialysis patients. Clinics, 70(5), pp.363-368.
- Scribner BH, Buri R, Caner JE, Hegstrom R, Burnell JM: The treatment of chronic uremia by means of intermittent hemodialysis: a preliminary report. Trans Am Soc Artif Intern Organs 6:114-122, 1960
- Siew, E. and Ikizler, T. (2010). Insulin Resistance and Protein Energy Metabolism in Patients with Advanced Chronic Kidney Disease. Seminars in Dialysis, 23(4), pp.378-382.
- Tedla, F., Brar, A., Browne, R. and Brown, C. (2011). Hypertension in Chronic Kidney Disease: Navigating the Evidence. International Journal of Hypertension, 2011, pp.1-9.
- The National Kidney Foundation. (2017). Understanding Your Lab Values. [online] Available at: https://www.kidney.org/atoz/content/understanding-your-lab-values
- US Renal Data System. Excerpts from the USRDS 2006 Annual Data Report. Am J Kidney Dis 49(Suppl 1), S1-S296, 2007
- World Health Organization. (2016). What is malnutrition?. [online] Available at: http://www.who.int/features/qa/malnutrition/en/
- Yap, H., Pang, S., Tan, C., Tan, Y., Goh, N., Achudan, S., Lee, K., Tan, R., Choong, L. and Chong, T. (2018). Catheter-related complications and survival among incident hemodialysis patients in Singapore. The Journal of Vascular Access, p.112972981876505.
- Zanchi, A., Tappy, L., Lê, K., Bortolotti, M., Theumann, N., Halabi, G., Gauthier, T., Mathieu, C., Tremblay, S., Bertrand, P., Burnier, M. and Teta, D. (2014). Pioglitazone Improves Fat Distribution, the Adipokine Profile and Hepatic Insulin Sensitivity in Non-Diabetic End-Stage Renal Disease Subjects on Maintenance Dialysis: A Randomized Cross-Over Pilot Study. PLoS ONE, 9(10), p.e109134.
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Cancer"
Cancer is a disease in which cells grow or reproduce abnormally or uncontrollably. Cancerous cells have the potential to spread to other areas of the body in a process called metastasis.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: