Adding Pleasurable Activities as an Effective Behavioral Intervention to Increase Positive Mood
Info: 7590 words (30 pages) Dissertation
Published: 25th Feb 2022
Tagged: Psychology
Abstract
Research has identified a number of psychological risk factors associated with persistent negative mood. The present case study examines the effect of behavioral interventions on increasing positive mood in a 25-year-old Caucasian female, currently working full time and enrolled in a doctoral level graduate program. Following an ABAB design, the study employed activity scheduling, addition of pleasurable activities, mood ratings, self-monitoring, and prompting to increase the individual’s positive mood. Each baseline and intervention phase lasted seven days. During the treatment phases, the participant scheduled the week’s activities, inputted them into her Google calendar, and received prompts to engage in the pleasurable activities via her Apple watch. Results indicated that her negative mood decreased, and her positive mood increased during the intervention phases compared to the baseline phases, an outcome most likely enhanced by the use of effective behavioral interventions and the participant’s high motivation and commitment.
Introduction
According to Lewinsohn et al. (1993) there are several assumptions regarding the behavioral theory of depression. A major assumption states that a low rate of response-contingent positive reinforcement has the tendency to act as an unconditioned stimulus for some depressive symptoms, such as fatigue, dysphoria, or other somatic symptoms (Lewinsohn et al., 1993). Behavioral theory states that the differences between a depressed and non-depressed individual lie in the differences in the number and kinds of reinforcing activities a person engages in, and the possibility that depressed individuals have higher rates of being in situations which lack reinforcement for them (Lewinsohn et al., 1993). Furthermore, the degree to which an individual’s behavior is maintained by reinforcement, is considered to be the antecedent condition for depression (Lewinsohn et al., 1993). If depression is to be avoided, the occurrence of behavior followed by positive reinforcement is essential, and the probability of depression occurring decreases when an individual’s behavior will be followed by reinforcement (Lewinsohn et al., 1993).
Depression can occur in any individual. It can be especially prevalent for those in graduate school or higher education due to the demands (Levecque, Anseel, Beuckelaer, Van der Heyden, & Gisle, 2017). The prevalence of mental health problems is higher in PhD students, with one in two PhD students experiencing psychological distress, and one in three at risk of developing a common psychiatric disorder (Levecque et al., 2017). Due to the heightened concerns and risks doctoral students experience it is necessary to gain a deeper understanding of the underpinnings and causes of depressive symptoms and psychological distress. Further research will allow clinicians and professionals to identify the symptoms, triggers, and potential forms of intervention for those who struggle with depression.
Beck’s cognitive model and subsequent theory states that negative self-schema involving dysfunctional and maladaptive beliefs about one’s self underlies vulnerability to depression (Mongrain & Blackburn, 2006). In several studies, research has shown that in a graduate student sample, perfectionistic beliefs and a negative inferential style were associated with a more chronic history of decreased mood and depression (Mongrain & Blackburn, 2006). Specifically, a negative inferential style for academic failure is increasingly common in graduate students and significantly increases students’ risk for depression and decreased mood (Mongrain & Blackburn, 2006). This information is especially pertinent as the case study focuses on a graduate student enrolled in a doctoral level program, where stressors are at an all-time high.
Research supports the effectiveness of Behavioral Activation employed in increasing an individual’s mood. Behavioral Activation, is an evidence-based treatment that focuses on identifying and scheduling enjoyable and meaningful activities to reduce one’s depression or negative mood, while also trying to address the obstacles or avoidance to participating in said activities (Haynes et al., 2018). Behavioral activation protocols often provide individuals with education around negative mood and depressive symptoms, how to identify pleasurable activities, how to schedule the activities, and how to notice and address the avoidant behaviors that often act as barriers to engaging in the enjoyable activities (Haynes et al., 2018). It aims to enhance environmental positive reinforcement for healthy and adaptive behavior, and works to decrease unhealthy behavioral avoidance through a functional analysis and use of specific strategies (Farchione, Boswell, & Wilner, 2017). By helping individuals experience first-hand how their environment plays a role in the maintenance of their negative mood, and that specific target behaviors can be strategically identified and modified, individuals’ self-esteem and self-efficacy often increases and subsequently, symptoms are reduced (Farchione, Boswell, & Wilner, 2017). Behavioral activation has been found to be helpful across a wide variety of settings with a diverse group of clinical populations.
In order to understand the Behavioral Activation model, one must also understand behavioral avoidance and how it plays a role in one’s mood. According to Jacobsen, Martell, and Dimidjian (2001), avoidance behaviors reduce an individual’s opportunities for reinforcement from the environment, requiring treatment to increase the persons’ awareness and insight into avoidance patterns and replace them with approach behaviors. In turn, this creates opportunities for positive reinforcement (Jacobsen, Martell, & Dimidjian, 2001). Psychoeducation is a crucial component in behavioral activation, by assisting individuals in better understanding how thoughts and behaviors are connected, and how engagement with certain behaviors has a direct link to their mood.
The literature suggests utilizing Behavioral Activation as a positive intervention for increasing an individual’s mood. A component of Behavioral Activation includes adding and scheduling pleasurable activities. Behavioral Activation is crucial when treating depression because the disorder can disrupt activities and daily routines (Markowitz, 2003). Behavioral Activation encourages individuals to broaden their behavioral experiences in the environment, increasing positive reinforcement and mastery though the addition of pleasurable activities (Markowitz, 2003). Several studies have supported this claim that there is an association between rate of positive reinforcement through pleasant events and activities and the intensity of depression (Lewinsohn et al., 1993).
Berenbaum (2002) conducted research focused on better understanding pleasurable activities, and how individuals come to experience positive emotions or feelings related to the activity. Berenbaum (2002) utilized a sample of college students, requesting the participants list activities that they found to be pleasurable and provide ratings as to how much the activities led them to feel different joy-related pleasurable feelings. The results demonstrated there were three identifiable types of pleasurable feelings: cheerfulness, contentment, and enchantment (Berenbaum, 2002). Berenbaum (2002) went on to explain the multitude of different activities that can yield positive emotions for people, including categories around “pleasures of the mind,” interests, musical and religious experiences, and social interactions. Part of the reason individuals find different activities enjoyable is because each individual regulates their emotions differently (Burr, Javiad, Jell, Werner-Seidler & Dunn, 2017).
Understanding the strategies to help build positive emotions may help to alleviate some of the stress and negative emotionality people experience on a daily basis (Burr et al., 2017). Additionally, increasing positive emotions will help to reduce a number of mental health conditions including anhedonia, depression, and social phobia (Burr et al., 2017). The way in which individuals understand and appraise their experiences during positive activities may impact their affect and overall mood (Burr et al., 2017). For example, if an individual is experiencing a positive mood, they might tend to focus on the fact that it will not last forever, or what are the bad things to follow, and this is likely to reduce their positive mood (Burr et al., 2017). On the other hand, if individuals take note of how good they feel, relate it to a personal quality, and savor the feelings, it is likely to increase their positive affect (Burr et al., 2017). A central focus in the clinical psychology field, and a target of treatment is to help individuals identify, target, and decrease thoughts that lead to the premature ending of positive and pleasurable activities and emotions (Burr et al., 2017).
Activity scheduling is an integral part of behavioral activation and typically serves two functions: to provide information regarding an individual’s baseline activity levels and mood and second, to demonstrate to an individual that there is a meaningful relationship between activity and mood (Kanter, Manos, Bowe, Baruch, Busch & Rusch, 2010). A number of aspects of our behavior can be better understood with an activity chart. For example, one can identify an individual’s general activity level, avoidance behaviors, moods associated with different activities, and consistency of activities and schedule keeping (Kanter et al., 2010). Therefore, activity monitoring is not a behavior change by itself, but rather, an assessment to support and rationalize behavior change, and a crucial precursor to any behavior changing efforts (Kanter et al., 2010). The research has indicated that behavior monitoring, on its own, positively impacts outcomes, and has been shown to decrease problematic behaviors (Kanter et al., 2010). Furthermore, activity monitoring has been used to facilitate cognitive restructuring, leading to a decrease in depressive symptoms, and increase in positive activity and affect (Kanter et al., 2010).
Activity scheduling is a crucial component of Behavioral Activation because it encourages individuals to approach activities that they may typically avoid, and assists individuals in analyzing the function of cognitive processes that serve as a form of avoidance (Veale, 2008). Fester (1973) developed a model of depression based on learning theory which argued that when people become depressed, their activities function as avoidance and escape from negative thoughts, feelings, or situations. As a consequence, an individual with depression may engage less frequently in pleasant or satisfying activities, and therefore will obtain less positive reinforcement than someone who does not have depression (Veale, 2008). Behavioral Activation does not just focus on activity scheduling but rather on the whole event and variables that influence unhelpful responses, seeking to identify what reinforcers predict and maintain the unhelpful responses (Veale, 2008). In addition to activity scheduling, Behavioral Activation protocols emphasize mood monitoring and encourage individuals to monitor the effect of their scheduled activities on their mood (Veale, 2008).
Studies have found that underlying symptoms of depression may represent a core set of vulnerabilities in an individual (Barlow, Sauer-Zavala, Carl, Bullis, & Ellard, 2014). This may include a tendency to experience negative emotions more intensely than others, paired with a propensity to evaluate things negatively, which in turn increases efforts to suppress these negative emotions and experiences, ultimately encouraging the emotions the return even more intensely (Rassin, Murris, Schmidt, & Merckelbach, 2000). With depression, one often sees individuals trying to cope with the negative and unpleasant emotional states by withdrawing and isolating themselves from activities and positive social interactions (Farchione, Boswell, & Wilner, 2017). Additionally, individuals often state that they do not have enough time to engage in pleasurable activities, when in actuality, they just are unable to appropriately schedule and complete them. Finally, avoidance may serve to reduce the negative emotions, but long term only contributes to the maintenance of the emotions and difficulties in regulating one’s emotions (Farchione, Boswell, & Wilner, 2017). Given the withdrawal from activities and tendency to avoid, Behavioral Activation components of activity scheduling and mood monitoring are essential.
The present study examines the effectiveness of behavioral interventions on increasing positive mood in a doctoral level graduate student. Research has identified the benefits of engaging in pleasurable activities as it relates to an increased positive mood. Additionally, data has been collected to demonstrate the benefits of Behavioral Activation and the scheduling of pleasurable activities. As revealed in previous research, self-monitoring, Behavioral Activation, and scheduling of activities have been shown to be effective in increasing a target behavior. Therefore, it is hypothesized that the participant’s mood will be more positive on days when they employ self-monitoring, Behavioral Activation, prompting, and the scheduling of pleasurable activities than on the days with no scheduled activities. Additionally, during the intervention phase, the participant will overall rate a more positive mood in comparison to the baseline phase’s reported mood levels.
Methods
Participant
The participant is a 25-year-old single Caucasian female who wishes to increase her positive mood. She is a second year graduate student in the clinical psychology doctoral program at the Philadelphia College of Osteopathic Medicine, and is participating in this study to fulfill a requirement for her Behavior Therapy course. The participant reports frequent headaches, and periods of low mood, attributed primarily to her full time professional and academic responsibilities. The participant reported her negative mood patterns began around a year ago. She reports an overall good physical health, but acknowledges she would like to improve her mental health.
Measurements
Mood Scale
The participant completed a 5-point Likert scale (1 = Strongly Disagree, 5 = Strongly Agree) each evening at roughly 10:00 p.m. to measure her mood. The scale sought to measure the participant’s perception of mood by asking her to rank her agreement or disagreement with ten mood descriptive words. For the purpose this case study, negative and positive mood ratings garnered the most attention. See Appendix A.
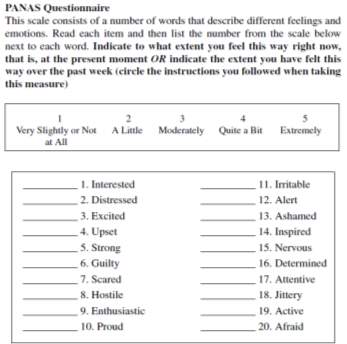
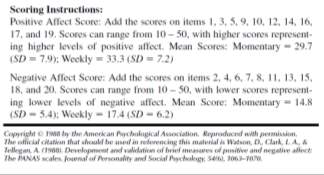
Positive and Negative Activation Schedule (PANAS)
The participant completed the PANAS, a 20-item scale that obtains separate measures of both positive and negative affect by utilizing a 5-point measuring scale (1 = Very slightly or not at all, 5 = Extremely). The 20-item scale is an abbreviated version of the PANAS full scale, and deemed most applicable for the current study. Reported by Watson (1988) the reliability and validity of the scale was moderately good. For the positive affect scale, the Cronbach alpha coefficient was 0.86 to 0.90, and the negative affect scale was 0.84 to 0.87 (Crawford & Henry, 2004). The PANAS scale has strong reported validity with measures such as distress, depression and anxiety (Crawford & Henry, 2004). See Appendix B.
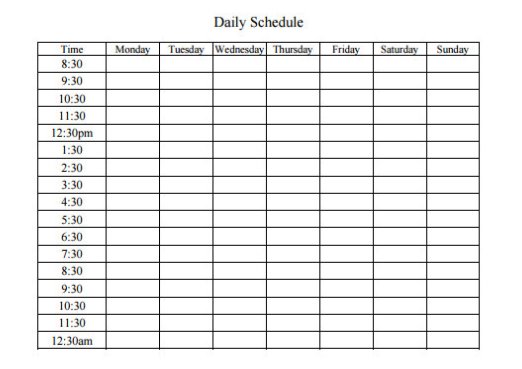
Activity Schedule
The participant utilized an activity schedule to coordinate and plan her activities for the intervention phases. She was instructed to choose a minimum of two enjoyable activities, for a minimum of 15 minutes each, for the five days out of seven during the intervention phase. Activities the participant chose include: knitting, reading a book for enjoyment, writing a blog post, journaling, meditating, listening to music, or going for a walk.
Apple Watch
After scheduling her activities on paper, the participant logged her schedule into a Google calendar, where reminders would be set though her Apple watch which she wore daily. She received a vibration reminder through her watch, five minutes before the activity and one minute before the activity was scheduled.
Procedure
This case study follows a single subject, single case, ABAB design. The first set of baseline data was collected for seven days until a data trend was determined. Then the first seven-day intervention phase began, followed by seven days of the return to baseline condition, followed by another seven-day intervention phase. During the baseline periods of the study, the participant was asked to go about her daily life with nightly mood checks utilizing the Mood scale and PANAS questionnaire. The participant was told to follow her typical daily activity regimen, not adding any enjoyable activities to enhance her mood.
During the intervention phases, the participant scheduled pleasurable activities for five of the seven days of the week, and utilized an activity scheduling chart to ensure she knew when and what activities in which to engage in. The activities were scheduled on the Sunday morning of the week, and scheduled for the following seven days. Activities that were scheduled included: knitting, reading a book for enjoyment, writing a blog post, journaling, meditating, listening to music, watching TV, or going for a walk. She was instructed to choose a minimum of two pleasurable activities per day for at least 15 minutes per activity, for the five days during the intervention phase. Additionally, once she scheduled on paper her activities for the week, she would input them to her Google calendar and set reminders to appear on her Apple watch, prompting her to engage in the activities. See Table 1 for schedule of activities for intervention conditions 1 and 2. She reported that she enjoys a routine and therefore scheduled similar times for her activities each day. On Sunday she scheduled 30 minutes of knitting from 8:00 a.m. to 8:30 a.m., 30 minutes of blogging from 5:00 p.m. to 5:30 p.m., and 30 minutes of reading for enjoyment from 9:00 p.m. to 9:30 p.m. On Monday she scheduled 20 minutes of walking outside from 7:30 a.m. to 7:50 a.m., 60 minutes of watching T.V. from 8:00 p.m. to 9:00 p.m., followed with reading for enjoyment from 9:30 p.m. to 10:00 p.m. before completing her mood scales and going to bed. On Tuesday she scheduled 20 minutes of walking outside from 7:30 a.m. to 7:50 a.m., 30 minutes of blogging from 12:30 p.m. to 1:00 p.m., and knitting that evening for 60 minutes from 8:00 p.m. to 9:00 p.m. On Friday and Saturday she scheduled 45 minutes of walking outside from 7:00 a.m. to 7:45 a.m., watching T.V. in the evenings from 7:00 p.m. to 8:00 p.m., and reading for enjoyment from 9:00 p.m. to 10:00 p.m. Each night of the week she recorded her mood by using her self-created Mood Scale and the PANAS scale, regardless of whether not the day involved the addition of pleasurable activities.
After one week of intervention, the participant returned to collecting baseline data once more as she returned to her daily life without the addition of the activity scheduling. Baseline data was collected and recorded for seven days. Finally, the last step of the intervention was implemented with the same procedures as the previous intervention for another seven days. Again the second intervention phase was followed with a second baseline phase and data collection.
Conceptualization
The participant in this study is a 25-year-old female who reports overall good physical health, with a slight decline in mental health due to increased pressures from school and work. The participant reports that her mental health began to dip during the first year of her doctoral program, as she began to take on more responsibilities in her professional work. She has no significant physical or mental diagnoses affecting her health. She reports that depression runs in her family, but does not feel as though she would meet criteria for any mood-related disorder. She denies any past or present suicidal or homicidal ideation. She attributes her negative mood to the stressors in her life and lack of time for enjoyable activities. She reports a history of seasonal allergies for which she takes Zyrtec. She denies any additional medications. She reports that she does not exercise as much as she would like, eats a balanced nutritious diet, and maintains an average weight. The participant denies any recent changes in her sleep or diet, and reports that she sleeps an average of seven hours a night. She does report that she has difficulty falling asleep, but once asleep experiences no issues. She reports that most nights she struggles to fall asleep due to the stressors in her life and things occurring in her mind. The participant reports it is hard to relax in the evenings and fall asleep, especially after she has classes that end late in the evening. Laying down in her bed after classes serves as an antecedent for negative mood and arousal as she begins to think about the day and all she has to do during the next day. Additionally, she reports checking her email as a precursor to feeling down as often it is full of tasks, assignments, or concerns to be handled. Checking her email and trying to go to sleep set the stage for the participant to experience a negative mood.
Functional Analysis
Following the seven-day baseline phase, a functional behavioral analysis was conducted to better understand conditions related to the participant’s current mood. Completion of this analysis offers a comprehensive understanding of the antecedents and the factors maintain the participant’s negative mood. The findings of the analysis are helpful in creating a multidimensional and individualized behavioral intervention plan for the participant. The possibility of effective reinforcers was also identified. The participant reports that when she has more time to engage in positive and fun activities, she feels better and has more energy, which positively reinforcers her to engage in more activities to continue feeling more positive. The participant reports that she wants to feel more positive and enjoy life more, and notices she experiences these feelings when she has more time for pleasurable activities, and makes a conscious effort to schedule and engage in them.
It is determined that the participant reports a more negative mood when she does not engage in any pleasurable activities, rating herself as more helpless, distressed, irritable, stressed, and negative on both the Mood scale and PANAS scale. It is identified that on the evenings when she has classes, she reports higher levels of irritability and stress. It is also identified that during the baseline ratings, the participant rated her days as more negative than during the intervention phases.
Further analysis identified that the consequence for not engaging in pleasurable activities, as evidenced by the baseline scores, was an overall lower reported mood, and feelings of irritability, distress, hopelessness, and helplessness. As a response to these symptoms, the participant reports more of a difficulty falling asleep, as she tends to focus on the many negative components in her life.
The participant reports that her parents have both struggled with depression at different time periods in their life. She also reports that during middle and high school she experienced feelings of hopelessness and distress when overwhelmed by athletics and academics. She reports having spoken with school counselors before, having noted that often the feelings subside when the environmental stressors decrease. She reports that she has been classified by some as a pessimist at times, but would consider herself a realist, noting that the world is not always a happy or positive place. She does also report that she wants to experience a more positive mood, and recalls fondly the days and times where her mental health has been excellent. She indicates that she was successful in adding and increasing the pleasurable activities as she genuinely wants to engage in those activities, yet often uses the excuse that there is not enough time.
Further conclusions from the analysis include that the participant’s ratings of negative mood and lack of interest in engaging in pleasurable activities may be present due to an underlying depressed affect where she does not have the energy to schedule activities and engage in them. Additionally, of note, the participant’s mood ratings where significantly more negative when she had classes at school, whereas on the evenings she did not, her mood ratings were slightly higher and more positive. Due to an inadequate stimulus control, the participant experienced a more negative mood responding to one stimulus (classwork and assignments) then with a different stimulus (work setting).
Based on the functional behavioral analysis, this study is designed to increase the participant’s daily positive mood ratings by adding pleasurable activities into her schedule. An Apple watch reminder will also prompt the participant when it is time to engage in an activity that she pre-scheduled for the week. Finally, the participant is asked to self-monitor and record her mood each night, which as previous research has shown will allow her to see trends and gain insight into her mood and affect.
Results
The results of this study indicate that there was an increase in positive mood during the intervention phases compared to the baseline phases as shown in Figures 1 and Figures 2, as measured specifically by the Mood scale, positive and negative mood ratings. The PANAS scale also displayed an increase in positive mood-related symptoms and decrease in negative mood-related symptoms during intervention phases. On the mood scale during the first baseline phase, the mean score for self-reported negative feelings was 3.9 per day with a standard deviation of 1.27, and the mean score for self-reported positive feelings was 3.0 per day with a standard deviation of 0.82. During the first intervention phase when the participant added pleasurable activities to her schedule, the negative feelings decreased to daily mean of 3.0 with a standard deviation of 0.82, and positive feelings increased to mean of daily rating 4.0 with a standard deviation of 0.87.
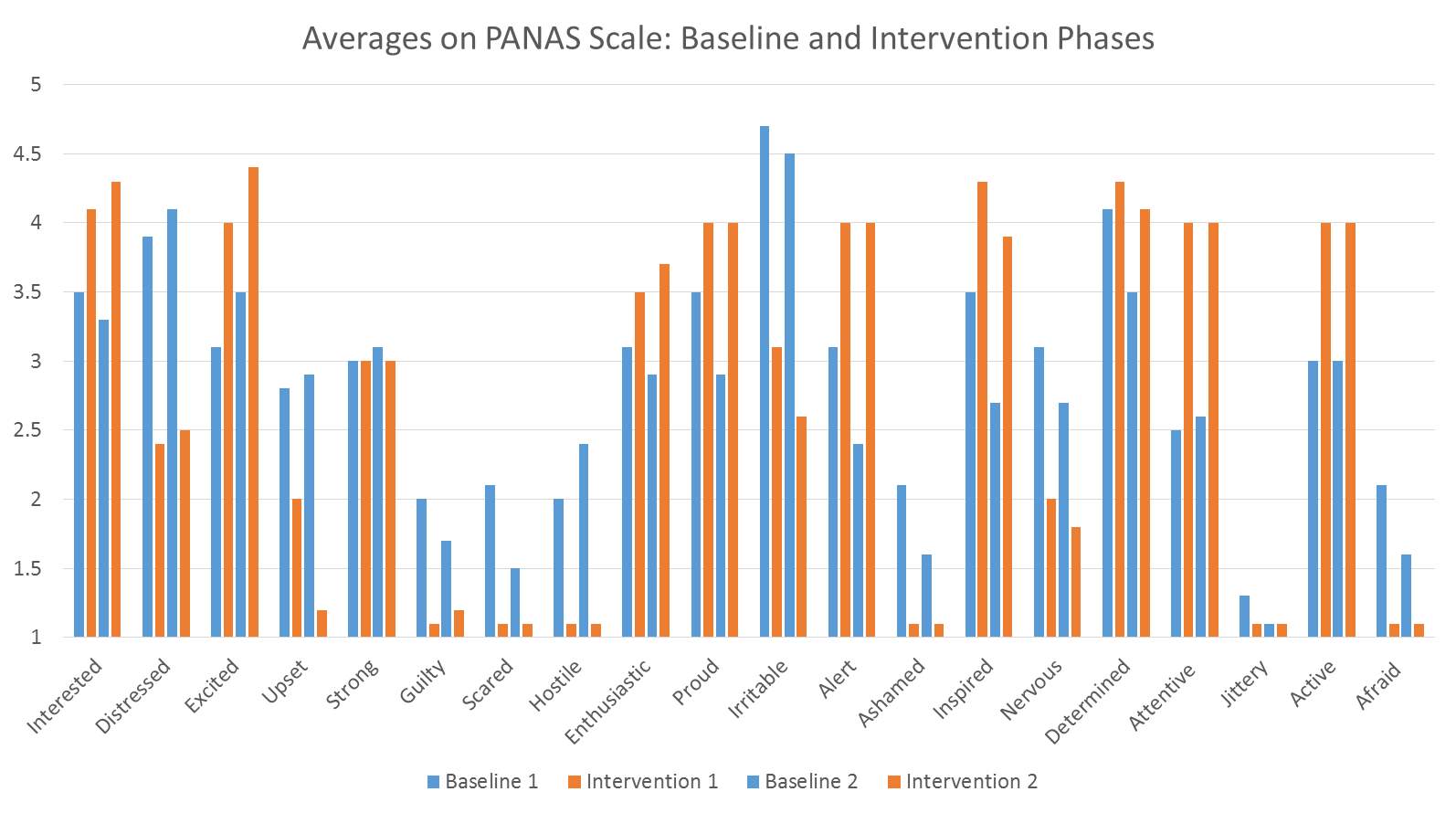
On the PANAS scale during the first baseline phase, the mean daily score for distressed feelings was 3.9, irritability was 4.7, and excitability was 3.1. After the intervention phase of adding pleasurable activities to her schedule, the participant’s mean score of distressed feelings decreased to 2.4, irritability decreased to 3.1, and feelings of excitability increased to 3.4.
The third phase of the experiment was a return to baseline where scores remained relatively consistent with the first baseline measures. For example, on the Mood scale, negative feelings received an average score of 4.0 per day (SD = 1.32), while positive mood received an average score of 3.4 per day (SD = 1.31). On the PANAS scale, irritability received an average score of 4.5, distressed received a 4.1 average score, and interested received an average score of 3.3. The second and final intervention phase was once again implemented and the participant’s positive mood scores increased, and negative mood scores decreased. On the Mood scale, the daily average score for positive mood increased to 4.0 with a standard deviation of 1.49, and negative mood daily score decreased to 2.6 with a standard deviation of 1.20. Regarding the PANAS scales, irritability decreased to an average score of 2.6, distressed decreased to an average score of 2.5, and enthusiastic increased to an average score of 3.7. The results of this study indicate an increase in self-rated scores of positive mood and a decrease in self-rated scores of negative mood during the intervention phases compared to the baseline phases, suggesting that the behavioral intervention contributed to increases in the participant’s positive mood.
Discussion
The present study’s purpose was to determine the effectiveness of behavioral interventions on increasing positive mood in a graduate student. As hypothesized, the results of this study indicate in increase in self-rated scores of positive mood and a decrease in self-rated scores of negative mood during the intervention phases compared to the baseline phases, demonstrating that the behavioral intervention implemented successfully increased the targeted behavior of increasing the participant’s positive mood. The findings were most likely due to a number of factors including Behavioral Activation, self-monitoring, activity scheduling, and mood ratings. Research has identified the benefits of engaging in pleasurable activities as it relates to an increased positive mood. Additionally, studies have demonstrated the benefits of Behavioral Activation and the scheduling of pleasurable activities.
The findings from the current study were consistent with previous studies, regarding the effectiveness of using Behavioral Activation, activity-scheduling, self-monitoring and mood ratings to increase an individual’s positive mood by adding pleasurable activities (Kanter et al., 2010). The literature supports the notion that those who engage in mood-related pleasant activities, measured by daily activity monitoring and mood ratings will experience an improved mood (Graf, 1977). Activity scheduling as a behavioral intervention may also be seen as a form of stimulus control, and has been found to act as a prompt in the environment to remove problem behaviors, such as rumination, insomnia, or addictive behaviors (Witkiewitz & Marlatt, 2004). The participant in the study acknowledged that, at times, she experienced difficulty falling asleep due to the cognitions and stressors she would focus on immediately before bed. Due to this, she intentionally scheduled evening pleasurable activities in hopes that it may take her mind off of the stressors and negativity, and increase her positivity and relaxation. A limitation of the current study is that no measures examining sleep were utilized, so it is unclear as to whether or not the activity scheduling assisted in sleep or induction of relaxation. For a future study, one may consider adding a sleep measure to identify if the activity scheduling and engagement with pleasurable activities may aid in sleep and ability to fall asleep.
Further limitations of the study include the short length of both the baseline and intervention phases. If the study were to be replicated, increasing the length of time for both the baseline and intervention phases would be recommended. A third limitation includes the potential confirmation bias of the participant who was aware of the hypotheses and goals in adding the scheduled pleasurable activities, and may report her moods inaccurately. Given the short length of time and individual participant, the study is not generalizable to the general public. Future studies should include a larger sample, and longer period of time. For example, a multiple baseline design with several graduate students, over a specific period of time could be utilized to compare and contrast how adding pleasurable activities affects their mood.
The specific components of Behavioral Activation are available in several manuals (Martell et al., 2001; Lejuez, Hopko, and Hopko, 2001; Addis and Martell, 2004), and one component consists of the scheduling of pleasant activities. According to the American Psychological Association, behavioral activation can help individuals to incorporate pleasurable and enjoyable activities into their daily lives (American Psychological Association, 2009). Given that the current participant experienced a negative mood due to stress and lack of time for pleasant activities, it was imperative that enjoyable activities and behavioral activation modules be implemented. The research supports the enhancement of mood through activities and considers behavioral activation to be efficacious as a form of treatment or intervention (Cuijpers et al., 2007; Ekers et al., 2008; Mazzucchelli et al., 2009).
Given the fact that the participant was a current doctoral student, understanding her stressors and mood is important to the field of higher education and those interested in working with graduate students. For example, recognizing that students do not feel they have adequate time for self-care is important if you want to promote the well-being of your students. Once recognized, professors and faculty can work with students to create a list of activities they enjoy as well as a schedule for the activities. Given the data which supports the use of Behavioral Activation, addition of pleasurable activities, and mood ratings, academic institutions may wish to take this under consideration when creating students’ schedules, or homework assignments. Courses could include requirements around self-care and pleasurable activities to ensure students are making the time for them. Additionally, the current data is crucial to understand if we want to better recognize the underpinnings of depression and other mood disorders correlated with a negative mood. Incorporating pleasurable activities in treatment for those with depression is useful and encouraged.
The implications of this study include better understanding negative mood and potential causes of depression, recognizing the need for pleasurable activities among graduate students, and the potential effects lack of positive mood and activities can have on one’s sleep and overall well-being. Future studies should include a larger sample and greater length of time to ensure results are generalizable. Additionally future studies could include different combinations of behavioral interventions in order to tease apart the effectiveness of each, rather than viewing them as a collection. Lastly, studies could collect data post-intervention in order to assess the long-term effectiveness of the behavioral intervention. For example, did this individual experience increased positive mood after the four week period? No information was collected on whether she continued adding pleasurable activities to her schedule, and setting reminders through her watch after the study’s conclusion. Gathering the data would only benefit future studies and consumers of research.
This study is an example of a successful integration of behavioral intervention to increase one’s positive mood, and decrease negative mood in a healthy adult female graduate student. The study demonstrated that behavioral interventions including self-monitoring, mood checks, activity scheduling, and adding pleasurable activities appears to be effective in increasing positive mood in an individual who reports to often struggle with negative mood, thus reducing possible health risks and symptoms associated with depressed mood.
Appendices
Mood Scale…………………………………………………………………Appendix A
PANAS Questionnaire…………………..………………………………….Appendix B
Activity Schedule…………………………………………………………….Appendix C
Appendix A
| Currently I feel… | 1-Strongly Disagree | 2- Disagree | 3- Neutral | 4- Agree | 5- Strongly Agree |
|
|||||
|
|||||
|
|||||
|
|||||
|
|||||
|
|||||
|
|||||
|
|||||
|
|||||
|
Appendix B
Appendix C
References
Addis, M.E., & Martell, C.R. (2004). Overcoming depression one step at a time: The new behavioral activation approach to getting your life back. New York: New Harbinger Press.
American Psychological Association (2009). Depression and how psychotherapy and other treatments can help people recover. http://ww.apa.org/topics/depress/recover.aspx#
Anderson, C. A., & Harvey, R. J. (1988). Discriminating between problems in living: An examination of measures of depression, loneliness, shyness, and social anxiety. Journal of Social and Clinical Psychology, 6,482-491.
Aspinwall, L. G., Taylor, S. E.(1992). Modeling cognitive adaptation: A longitudinal investigation of the impact of individual differences and coping on college adjustment and performance. Journal of Personality and Social Psychology, 63, 989-1003.
Atkinson, R. L., Atkinson, R. C., Smith, E. E., Bern, D. J., & Nolen-Hoeksema, S. (1996). Introduction to Psychology. (Translator: Yavuz Alagon). Ankara: Arkadas, Publishing.
Barlow, D. H., Sauer-Zavala, S., Carl, J. R., Bullis, J. R., & Ellard, K. K. (2014). The nature, diagnosis, and treatment of neuroticism: Back to the future. Clinical Psychological Science, 2, 344–365.
Barrett, L. F., & Russell, J. A. (1999). Structure of current affect. Current Directions in Psychological Science, 8, 10-14
Berenbaum, H. (2002). Varieties of joy-related pleasurable activities and feelings. Cognition & Emotion, 16(4), 473-494.
Burr, L., Javiad, M., Jell, G., Werner-Seidler, A., & Dunn, B. D. (2017). Turning lemonade into lemons: Dampening appraisals reduce positive affect and increase negative affect during positive activity scheduling. Behaviour Research And Therapy, 9191-101.
Crawford, J. R., & Henry, J. D. (2004). The positive and negative affect schedule (PANAS): construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43, 245-265.
Cuijpers, P., van Straten, A., & Warmerdam, L. (2007). Behavioral activation treatments of depression: A meta-analysis. Clinical Psychology Review, 27, 318-326.
Ekers, D., Richards, D., & Gilbody, S. (2008). A meta-analysis of randomized trials of behavioral treatments of depression. Psychological Medicine, 38, 611-623.
Farchione, T. J., Boswell, J. F., & Wilner, J. G. (2017). Behavioral activation strategies for major depression in transdiagnostic cognitive-behavioral therapy: An evidence-based case study. Psychotherapy, 54(3), 225-230.
Ferster, C. B. (1973) A functional analysis of depression. American Psychologist, 28, 857–870.
Graf, M. (1977). A mood-related activities schedule for the treatment of depression. Dissertation Abstracts Internation, 38, 1400-1401.
Haynes, T., Turner, J., Smith, J., Curran, G., Bryant-Moore, K., Ounpraseuth, S. T., & Yeary, K. K. (2018). Reducing depressive symptoms through behavioral activation in churches: A Hybrid-2 randomized effectiveness-implementation design. Contemporary Clinical Trials, 6422-29.
Heiman,T. (2004). Examination of the salutogenic model, support resources, coping style and Stressors among Israeli university students. The Journal of Psychology, 138 (6), 505-520.
Jacobson, N. S., Martell, C. R., & Dimidjian, S. (2001). Behavioral activation treatment for depression: Returning to contextual roots. Clinical Psychology: Science and Practice, 8, 255–270.
Lejuez, C.W., Hopko, D.R., & Hopko, S.D. (2001). A brief behavioral activation treatment for depression: Treatment manual. Behavior Modification, 25, 255-286.
Levecque, K., Anseel, F., Beuckelaer, A.D., Van der Heyden, J., & Gisle, L. (2017). Work organization and mental health problems in PhD students. Research Policy, 46 (4), 868-879.
Lewinsohn, P. M., Hops, H., Roberts, R. E., Seeley, J. R., & Andrews, J. A. (1993). Adolescent psychopathology: I. Prevalence and incidence of depression and other DSM-III—R disorders in high school students. Journal of abnormal psychology, 102(1), 133.
Markowitz, J.C. (2003). Depression in context: Strategies for guided action. The American Journal of Psychiatry, 160 (7)1366-1366.
Martell, C.R., Addis, M.E., & Jacobson, N.S. (2001). Depression in context: Strategies for guided action. New York: Norton.
Mazzucchelli, T., Kane, R., & Rees, C. (2009). Behavioral activation treatments for adults: A meta-analysis and review. Clinical Psychology: Science and Practice, 16, 383-411.
Mongrain, M., & Blackburn, S. (2006). Cognitive Vulnerability, Lifetime Risk, and the Recurrence of Major Depression in Graduate Students. Cognitive Therapy & Research, 29(6), 747-768.
Oerlemans, W. G., & Bakker, A. B. (2014). Why extraverts are happier: A day reconstruction study. Journal of Research In Personality, 5011-22
Polak, M. A., Richardson, A. C., Flett, J. A. M., Brookie, K. L., & Conner, T. S. (2015). Measuring mood: Considerations and innovations for nutrition science. In L. Dye, and T. Best (Eds.) Nutrition for Brain Health and Cognitive Performance (pp. 93 – 119). London, UK: Taylor and Francis
Rassin, E., Muris, P., Schmidt, H., & Merckelbach, H. (2000). Relationships between thought-action fusion, thought suppression and obsessive-compulsive symptoms: A structural equation modeling approach. Behaviour Research and Therapy, 38, 889–897.
Veale, D. (2008). Behavioural activation for depression. Advances in Psychiatric Treatment, 14(1), 29-36.
Waternman, A.S. (2005). When effort is enjoyed: Two studies of intrinsic motivation for personally salient activities. Motivation and Emotion, 29, 165-188.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063-1070.
Witkiewitz, K., & Marlatt, G.A. (2004). Relapse prevention for alcohol and drug problems: That was Zen, this is Tao. American Psychologist, 59, 224-235.
TABLE A
Mean and Standard Deviation of Mood Scale: Positive and Negative Mood
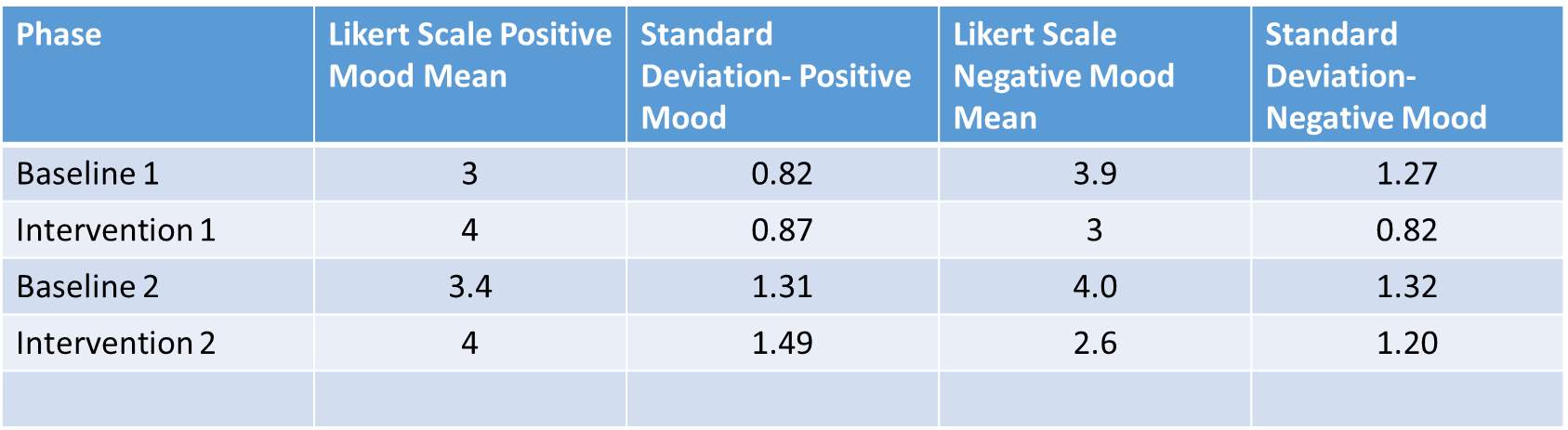
Table B
Average Mood Ratings on Mood Scale and PANAS Scale
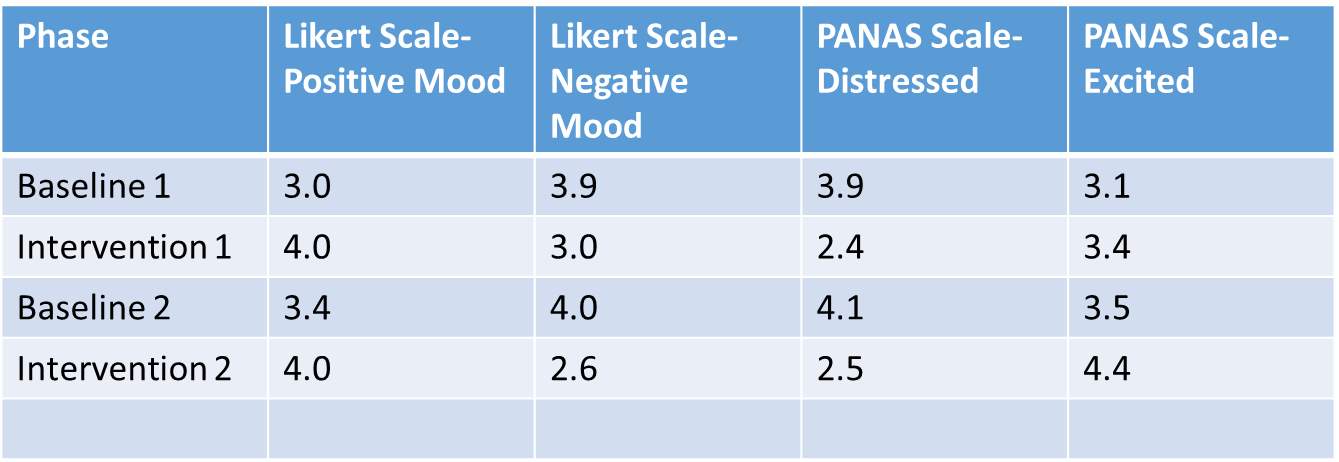
FIGURE 1
Averages of Mood Scale Scores: Baseline and Intervention Stages
0 = Strongly Disagree
5 = Strongly Agree

FIGURE 2
Averages on PANAS Scale: Baseline and Intervention Phases
1 = Very Slightly or Not at All
5 = Extremely
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Psychology"
Psychology is the study of human behaviour and the mind, taking into account external factors, experiences, social influences and other factors. Psychologists set out to understand the mind of humans, exploring how different factors can contribute to behaviour, thoughts, and feelings.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: