Alcoholism and Drug Dependence in Ireland: Study of Construction Workers
Info: 26955 words (108 pages) Dissertation
Published: 25th Nov 2021
Abstract
The impact of alcoholism and drug dependence in the workplace often focuses on premature death/fatal accidents; injuries/accident rates; absenteeism and loss of production. This can have a detrimental effect on construction sites. Many industry professionals suggest that substance abuse is prevalent on Irish construction sites from their experiences in the field. However, some believe it is a thing of the past and it is not a problem at present. Therefore, the purpose of this thesis is to to investigate and examine substance abuse and its presence in the Irish Construction Industry. This will be established through research and analysis of feedback from larger contractors and training services in the form of primary data.
The literature review provides a background to the thesis topic in the form of secondary research. This chapter covers all of the following areas that were applicable to the aim and objectives. This information was gathered through various books, publications, databases, academic journals and internet websites. Whilst the information is relevant to the thesis topic, it lacks statistics and specific information regarding the Irish construction industry itself. Hence, a number of interviews with industry professionals in Ireland were carried out in order to achieve this.
Five interviews as well as a focus group (3 members) were carried out within different companies in the Irish construction industry. The representatives were from two large Irish contractors (anonymous) as well as Salus training services. The data obtained from these interviews was used to validate and make comparisons between the literature review and the professional opinions
This thesis concludes on whether or not substance abuse is prevalent on construction sites in Ireland and reasons behind the verdict from both the primary and secondary research methods.
Abbreviations
SHWWA – Safety, Health and Welfare at Work Act 2005
HAS – Health and Safety Authority
WHO – World Health Organisation
NACDA – National Advisory Committee on Drugs and Alcohol
EMCDDA – European Monitoring Centre for Drugs and Drug Addiction
OECD – Organisation for Economic Co-Operation and Development
EU – European Union
AADAC – Alberta Alcohol and Drug Abuse Commission
UK – United Kingdom
USA – United States of America
UCATT – Union of Construction Allied Trades and Technicians
ILO – International Labour Organisation
BAC – Blood Alcohol Content
GHB – Gamma Hydroxybutyric
PCP – Phencyclidine
MDMA – Methylenedioxymethamphetamine
IOM – Institute of Medicine
OR – Odds Ratio
CIF – Construction Industry Federation
EAP – Employee Assistance Programme
CSAT – Center for Substance Abuse Treatment
MAST – Michigan Alcoholism Screening
AUDIT – Alcohol Use Disorders Identification Test
FORS – Fleet Operator Recognition Scheme
HSEQ – Health, Safety, Environmental and Quality
Table of Contents
Click to expand Table of Contents
Chapter 1 Introduction
1.1 Introduction
1.2 Aim and Objectives
Aim:
Objectives:
1.3 Thesis Summary
1.3.1 Chapter 1 – Introduction
1.3.2 Chapter 2 – Literature Review
1.3.3 Chapter 3 – Methodology
1.3.4 Chapter 4 – Analysis of Data and Findings
1.3.5 Chapter 5 – Conclusion and Recommendations
Chapter 2: Literature Review
2.1 Introduction
2.2 Definition of Substance Abuse
2.2.1 Drug
2.2.2 Drug Use
2.2.3 Drug Misuse
2.2.4 Abuse
2.3 Substance Abuse in Ireland
2.3.1 NACDA Survey of Drug Prevalence in Ireland 2014/15
2.3.2 Alcohol Consumption in Ireland
2.3.3 Prevalence of Substance Use in the Construction Industry
2.3.4 Forms of Substances and their effects
2.4 Substance Abuse Related Workplace Accidents
2.4.1 Reviews on Relationship between Substance Abuse and Misuse and Occupational Injuries
2.4.2 Alcohol Use and Occupational Injuries
2.4.3 Drug Use and Occupational Injuries
2.5 Employer’s and Employee’s duties in relation to drug use in Ireland
2.5.1 Employer’s and Employee’s duties
2.5.2 Disciplinary Procedure
2.6 Remedies and Actions of preventing Substance Abuse in the workplace
2.6.1 Treatment Recommendations
2.6.2 Workplace Policies and Drug Testing
2.6.3 Employee Assistance Programmes (EAP)
2.6.4 Health Plans
2.6.5 Workplace Health and Wellness Programmes
2.6.6 Treatment
2.6.7 Screening and Assessment
2.7 Case Study
2.7.1 ‘Spotlight On’ Scheme
Chapter 3: Methodology
3.1 Introduction
3.1.1 Aim of research
3.1.2 Research objectives
3.2 Research Strategy
3.3 Primary Research
3.2.1 Research design
3.2.2 Ethical considerations
3.2.3 Sample Frame
3.2.4 Sample size and Sampling strategies
3.4 Secondary Research
3.5 Interviewees:
Interviewee 1
Interviewee 2
Interviewee 3
Interviewee 4
Interviewee 5
3.5.1 Access
3.5.2 The Settings
3.6 Data collection
3.6.1 Procedure
3.6.2 Pilot study
3.6.3 Reflection on study process
3.7 Data analysis
Chapter 4: Analysis of Data and Findings
4.1 Introduction
4.2 Qualitative Findings
4.2.1 Past and Present
4.2.2 Suspicions of Substance Abuse on Site and Resulting Accidents
4.2.3 Link between accidents and alcohol/illicit drugs
4.2.4 Flaws in Safety, Health and Welfare at Work Act 2005
4.2.5 Lack of drug testing conditions in contracts
4.2.6 Substance use course of action
4.2.7 Workplace policies
4.2.8 Future Problems
4.2.9 Introduction of random drug testing in Ireland
4.3 Analysis
4.3.1 Prevalence of alcohol and drug use in the construction industry
4.3.2 Substance abuse-related workplace accidents
4.3.3 Employer and Employees duties regarding alcohol and illicit drug use in construction
4.3.4 Remedies and actions that may combat substance abuse
Chapter 5: Conclusion and Recommendations
5.1 Aim and Objectives
5.1.1 Aim of research
5.1.2 Research Objectives
5.2 Achievement of aim and objectives
5.3 Limitations during the Research
5.4 Recommendations
References
Interview Questions
Chapter 1 Introduction
1.1 Introduction
“Research has shown that groups of people who work together, whether in small teams or larger organizations, develop shared beliefs and practices that can influence alcohol use” (National Institute on Alcohol Abuse and Alcoholism, 2011).
In many occupations, this workplace culture can influence various beliefs including acceptable drinking contexts i.e. routine drinking with co-workers before, during and after work as well as their drinking behaviour i.e. the number of drinks they consume, showing the effects of alcohol, partaking in fights, arguing with their supervisors, sleeping on the job, coming into work hungover (Ames, Grube, & Moore, 1997) or in the construction world, operating plant such as excavators or tower cranes while under the influence.
As well as the alcohol drinking issue in the workplace, there are some concern with a new culture of personnel who have a desire or habit of using illicit drugs and over using prescribed medications. Management are confronted with the acknowledgement that the workforce on the site are affected by a licit or unlawful substance. Their concerns include the negative outcomes for the worker under the influence as well as the workers working around them, there may even be a loss of property i.e. site closure.
All drugs and substances are going to have some affect, good or bad on the person taking it whether it is injected or ingested. The consumption of illegal substances may lead to negative reactions to a person’s psychology, physiology or even both. When substances are combined with legal medications there is a higher risk of negative outcomes. Undesirable reactions are always a possibility when prescribed medications are mixed with over the counter medication such as painkillers and/or alcohol. Tinsley S. Harrison states that:
“Every drug can produce untoward consequences, even when it is used according to standard or recommended methods of administration.” (Harrison, 1950)
Over time, at a constant level of dosage or at a constant substance combination consumption, various substances, medical or illicit, will usually decrease its effectiveness as a result of a chemical tolerance built within the brain and central nervous system. However, the tolerance can potentially cause a higher craving for the substance. As a result, this can often lead to a self-dosage increase and potentially a higher probability of negative psychological or physiological reactions.
In an attempt to counter the lethal combination of a hazardous working environment with substance abuse, the Health and Safety Authority enacted a clause into the Safety, Health and Welfare at Work Act 2005 (SHWWA). This clause required submission by employees for appropriate tests for intoxicants in order to support employers to deal with the issue.
The clause reads:
“An employee shall, while at work if necessary required by his or her employer, submit to any appropriate, reasonable and proportionate tests for intoxicants by or under the supervision of a registered medical practitioner who is competent, as may be prescribed.”
(Health and Safety Authority, 2005)
This dissertation will give an overview of the drug problem in Ireland and investigate the risks it poses if at all on our construction sites. In addition, it will look at the employer’s rights when he/she believes a worker is under the influence as well as the various remedies and actions that could be used to combat the situation as well as look at the health and safety risks arising from this situation.
1.2 Aim and Objectives
Aim
The aim of this dissertation is to investigate and examine substance abuse and its presence in the Irish Construction Industry.
Objectives
- Investigate drug abuse in Ireland and the Construction Industry.
- Examine the substances most commonly associated with workplace related accidents.
- Detail the Employer’s position and legal duties in relation to substance abuse on Irish construction sites.
- Investigate and propose possible remedies/actions that can be taken to combat substance abuse on construction sites in Ireland.
1.3 Thesis Summary
1.3.1 Chapter 1 – Introduction
The first chapter introduces the dissertation topic and briefly explains prevalence of alcohol and substance abuse in the workplace along with the aim and objectives of the thesis topic.
1.3.2 Chapter 2 – Literature Review
This chapter contains current published literature about the thesis topic and other relevant material on the matter. This chapter begins with defining substance abuse. Following this is an investigation into drug abuse in Ireland, assessing the risks on site as a result, the employer’s rights framework and actions/remedies that can be taken to combat the situation. The researcher will then form a conclusion based on reviewing the existing literature.
1.3.3 Chapter 3 – Methodology
This chapter explains two methods of research employed by the researcher to gain an understanding of the thesis topic. The primary method of research was carried out through qualitative research interviews with relevant industry professionals. The secondary method of research was employed through a desk study of previous published literature.
1.3.4 Chapter 4 – Analysis of Data and Findings
This chapter reviews the findings and evaluates the industry’s opinions which have been obtained through the process of semi-structured interviews. The findings are then analysed in order for the researcher to achieve the set objectives, outlined in Chapter 1.
1.3.5 Chapter 5 – Conclusion and Recommendations
This chapter summarises the information collected from the primary and secondary data. Once the aim and objectives have been answered, the researcher will draw conclusions and make recommendations.
Chapter 2: Literature Review
2.1 Introduction
The literature review was used to establish a logical understanding of substance abuse and its effect on a person including those working in construction. The literature review was used as a secondary source of data to ensure the researcher has a complete understanding and knowledge of the topic. Additionally, it is used as a comparison for the primary data collected by the researcher. The areas the researcher has focused on are as follows: definition of substance abuse, drug abuse in Ireland, risks on site when substance abuse is a factor, the framework of employer’s rights and actions or remedies that may combat the situation.
2.2 Definition of Substance Abuse
2.2.1 Drug
A drug, in its broadest term is “any substance which changes the way the body functions, mentally, physically or emotionally.” (Eastern Regional Health Authority, 1997)
This definition does not discriminate between alcohol, caffeine, tobacco, over the counter drugs, prescribed drugs or illicit drugs. Instead it focuses on behavioural or body changes created as a result of the use of such substances. These particular substances are referred to as psychoactive drugs. This means the drug affects the central nervous system and alter mood, thinking, perception and behaviour. (Rassool, 1998)
2.2.2 Drug Use
Drug use is a broad term to cover the taking of all psychoactive substances within which there are various stages:
- Drug Free/Non-Use
- Experimental Use
- Recreational Use
- Harmful Use (Misuse/Dependence)
2.2.3 Drug Misuse
Royal College of Psychiatrists (Drug and Alcohol Review, 1987) define substance misuse as “any taking of a drug which harms or threatens to harm the physical or mental health or social well-being of an individual or other individuals or society at large, or which is illegal.”
2.2.4 Abuse
Substance abuse is described as a maladaptive pattern of substance use leading to clinically significant impairment or distress, demonstrated by any of the following within a one-year period:
- Recurrent use which leads to the failure of fulfilling major role obligations (work, home, school etc.)
- Recurrent use in situations where it is physically hazardous (drinking driving)
- Repeated substance related legal problems (drunken disorderly conduct)
- Persistent use despite recurrent social/interpersonal problems caused or provoked by the effects of substances. (e.g. physical/argumentative fights with spouse)
(American Psychiatric Association, 2013)
The World Health Organisation (World Health Organisation, 2013) defines substance abuse as “the harmful or hazardous use of psychoactive substances, including alcohol and illicit drugs. Psychoactive substance use can lead to dependence syndrome – a cluster of behavioural, cognitive, and physiological phenomena that develop after repeated substance use and that typically include a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal state.”
2.3 Substance Abuse in Ireland
2.3.1 NACDA Survey of Drug Prevalence in Ireland 2014/15
In 2002/03, the first national survey on drug use among the general population aged 15-64 of Ireland was carried out. (National Advisory Committee on Drugs and Alcohol, 2015) The results of the survey were published by the National Advisory Committee on Drugs and Alcohol (NACDA) and the Alcohol Information and Research Unit within the Department of Health, Social Services and Public Safety in Ireland. The survey was repeated in 2006/07, 2010/11 and 2014/15, interviewing 4,967, 5,128 and 7,005 respectively.
In 2014/15, the survey sampled a representative number of people aged 15+ years from August 2014 to August 2015 in Ireland. The survey was carried out according to standards set out by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). The date relating to drug prevalence was categorized into used in lifetime, within the last year and within the last month.
The survey was commissioned by the NACDA in Ireland. The survey’s main focus was to obtain prevalence rates for key illegal drugs. These drugs included cannabis, ecstasy, cocaine and heroin used in a lifetime, in the last year or month.
The survey questionnaire was based on guidelines the EMCDDA drew up. The questionnaires were carried out through face-to-face interviews with participants who lived in a household aged 15+ years. Therefore, anyone living in prison for example or 15-years did not participate. The survey results were split into three stages:
- Prevalence of Drug Use and Gambling in Ireland 15+ years;
- Prevalence of Drug Use and Gambling in Ireland by Age;
- Prevalence of Drug Use and Gambling in Ireland by Age and Gender.
The definitions of lifetime, last year and last month prevalence adopted for NACDDA‘s (2015) survey are as follows:
Prevalence: “the proportion of a population who have used a drug over a particular time period.”
Lifetime prevalence: “the proportion of the sample that reported ever having used the named drug at the time they were surveyed. A person who records lifetime prevalence may – or may not – be currently using the drug. Lifetime prevalence should not be interpreted as meaning that people have necessarily used a drug over a period of time or that they will use the drug in the future.”
Last year prevalence: “the proportion of the sample that reported using a named drug in the year prior to the survey.”
Last month prevalence: “the proportion of the sample that reported using a named drug in the 30-day period prior to the survey. Last month prevalence can be referred to as current use.”
The National Advisory Committee on Drugs and Alcohol (2015) concluded that 26.4% of the Irish adults surveyed report using an illegal substance in their lifetime. For the purpose of this thesis, lifetime use does not make for significant findings as it is too vague. To gain some more significant findings, this thesis focuses more on usage within the previous year or month in which the survey was carried out. The survey found that over the previous 12 months, 7.5% of adults used some form of illegal drug with cannabis being found to being the most commonly used as 6.5% of those surveyed admitting to its use. Cannabis appears to be used significantly more than ecstasy (1.8%), cocaine (1.3%) and cocaine powder (1.2%) which followed as the 2nd, 3rd and 4th most used drug available respectively.
In the previous month alone, 4% of adults had used a drug deemed to be illegal which equates to more than half of those who have used an illicit drug in the previous year. Alcohol consumption statistics are significantly high with 77% and 62.1% stating they had consumed alcohol in the previous year and month respectively.
The National Advisory Committee on Drugs and Alcohol (2015) survey found that illicit drug use was most prevalent amongst those aged 15-24 years old with 18.7% (previous year) and 9.6% (previous month) of young people stating they had used drugs. Alcohol usage was most common among 35-44 year olds. In the previous month, the majority (>50%) of age groups bar the 65+ group consumed alcohol.
It was found that in the previous year the use of illegal drug was highest among those aged 15-24 for both genders with males (25.4%) considerably higher than females (12%). The results showed that men used cannabis at least twice as much as women across most categories.
In the twelve months prior to the survey, alcohol consumption was highest among males aged 25-34 years, with 86.4% stating they had consumed alcohol in those months compared to the highest female age group of 35-44 years at 81.7%. Similar patterns could be seen for both genders in terms of previous month usage in the 15-24-year-old range with males significantly higher than females at 13.4% and 5.8% respectively.
The (2015) survey sought to compare the use of alcohol and drugs in the most up-to-date survey against the previous surveys carried out in 2002/03, 2006/07 and 2010/11. It found that in the previous year and month prevalence rose significantly since the release of the last survey (2010/11), respectively from 7% to 8.9% and from 3.2% to 4.7%.
The prevalence of cannabis usage in the year previous rose from 6.0% (2010/11) to 7.7% (2014/15), ecstasy use from 0.5% (2010/11) to 2.1% (2014/15).
It was found that significant increases in illegal drug use among 15-34 year olds over the previous year and month compared to that in 2010/11. The use of ecstasy in the year previous rose from 0.9% (2010/11) to 4.4% (2014/15) and from 0.1% (2010/11) to 2.1% (2014/15) in the last month.
The survey found that there had been an increase in illicit drug use among both genders in the previous year and month. This is the case both since the last study in 2010/11 and the first survey carried out in 2002/03.
2.3.2 Alcohol Consumption in Ireland
The Department of Health (2012) recognise that “that individuals are primarily responsible for their own behaviour, the State has a responsibility to preserve and protect public health and the general wellbeing of society.” Alcohol plays a significant role in Irish society. Between 1989 and 1999, Ireland had the largest increase in alcohol intake among all EU countries with an increase of 41% per capita. According to the Department of Health, alcohol is responsible for many of Ireland’s health and social harms in society and places a huge burden on the State’s resources in dealing with the consequences of alcohol use and misuse. A number of interventions are needed in order to reduce alcohol-related harm across the country. The World Health Organisation (2009) state that alcohol interventions that targeted vulnerable groups can prevent alcohol-related harm but policies targeted at the population as a whole, while having a protective effect on vulnerable populations, reduces an overall level of alcohol problems.
According to the Department of Health (2012) Irish adults drink more dangerously than that of any other country. The department found that the average Irish adult drank 11.9 litres of pure alcohol in 2010 which in context equates to 482 pints of beer, 125 bottles of wine or 45 bottles of vodka. Although the consumption of alcohol has reduced since 2000, adults in 2010 were drinking more than twice the average of alcohol consumed per adult in 1960. Similar findings were made by the OECD (2011) who found that Ireland’s alcohol consumption in 2009 per capita was 11.3 litres per adult (15+ years) which was the tenth highest of 40 countries that the report covered in 2009. The average amount of alcohol consumed in 2009 was 9.1 litres per adult. The European Commission (2010) found that Irish adults binge drink more than any other European country, with 25% of Irish adults reporting that they binge drink on a weekly basis. Over 50% of Irish drinkers identified themselves as having a harmful drinking pattern equating to c.1,500,000 Irish adults. Morgan (2009) found that Irish children are drinking from a younger age and drinking more than before.
The Healthy Ireland Survey (Department of Health, 2016) found that three quarters of the Irish population consumed alcohol in the last year. The results of the survey shown that 55% of drinkers, drink at least once a week, with those aged 55-64 drinking the highest weekly (66%). There was a significant difference between male and female whom are 35+ and drink at least once a week, 68% and 52% respectively.
During a typical drinking session, 37% of drinkers indicated that they drink six or more standard drinks. The majority of men who do drink, binge drink on a typical occasion (55%), far more than women with 1 in 5 drinking to this level. The majority (54%) of drinkers aged under 25 binge drink on a typical occasion, 67% in men and 39% in women.
The survey found that 97% of drinkers consider themselves to be light or moderate drinkers while a quarter of drinkers stated that they occasionally binge drink. 29% of people who do not class themselves as an occasional binge drinker drink six or more alcoholic drinks at least once a month. Despite binge drinking on a typical drinking occasion, 57% of drinkers aged under 25 consider themselves to be light drinkers.
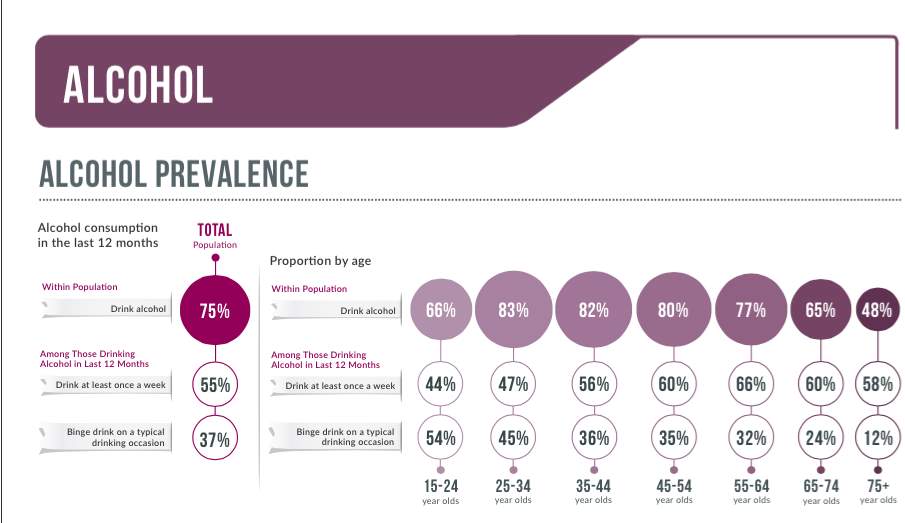
Figure 1 – Alcohol Prevalence in Ireland – Healthy Ireland Survey, 2016

Figure 2 – Description of own drinking behaviour – Healthy Ireland Survey, 2016
The Department of Health (2012) found that 4,321 deaths between 2004 and 2008 were due to either alcohol poisoning or deaths in alcohol dependent people, equating to 88 deaths each month in 2008. During the four-year period, alcohol cause nearly twice as many deaths as all drugs combined. While during 2000-2004, alcohol caused 4.4% (6,584) of deaths in Ireland including deaths as a result of accidental and non-accidental injuries that occurred to those under the influence of alcohol. (Martin, et al., 2010).
2.3.3 Prevalence of Substance Use in the Construction Industry
Construction Industry workers report higher than average rates of at-risk alcohol use, use of illicit drugs, use of tobacco and moderate or heavy smoking. The Alberta Alcohol and Drug Abuse Commission (AADAC) (2002) conducted a prevalence survey in which they found that the construction industry was regarded as a group of concern in terms of rates of substance use. Lipscomb & Li (2003) carried out a large work-group study in America between 1989 and 1998. Through this study they found that 6.6% of the workers had received a substance abuse-related diagnoses.
Smoking
Through a study of health interview data sets in the U.S, the highest smoking rates were reported in the construction industry with 39% revealing they smoked (Smith, 2008). Alvania, et al (2009) found that smoking was a factor in longer-term sick leave.
Alcohol
Through a national sample conducted by Larson, et al (2007) of full-time American workers aged 18-64, construction workers had the highest rate of past month alcohol use compared to workers in all other industries at 16%.
A survey carried out by Iacuone (2005) which took place in Victoria, Australia at several construction sites over a six month period found that the consumption of alcohol is an important aspect of male culture in the construction industry and that there is a certain pressure for a nondrinker to become a drinker. Data collected in 1997 in the US states that there was almost double the amount of heavy alcohol users among construction workers (12.4%) than the national average for other industries (7.6%) (Rountree, 2002). As well as this a Cundrai, et al (2009) survey conducted in the U.S. found that 17% of male construction workers surveyed could be designated as problem drinkers.
Illicit Drug Use
In 2002, it was estimated that 16,738 workers in Alberta used drugs while at work. While there was variation in the use of illicit drugs by industry and occupation, above average rates of drug use was reported in the construction industry (Alberta Alcohol and Drug Abuse Commission, 2002). This was similar to data cited by Rountree (2002) in which it was found that the percentage of illicit drug users among construction workers (14.1%) was double the national average for all industries (7.7%).
In March 2001, Mace’s site manager on the £250m SmithKline Beecham headquarters project in Brentford received anonymous phone calls warning him that drugs were being dealt on site.
He decided to contact the police who came to site and warned the 2000-strong workforce that they were being monitored and that undercover members of the police force would be trying to catch the dealers. The police as well as local anti-drugs campaigners came to site to give advice to workers about drugs and, together with Mace, made them aware of the dangerous risks drug use can have on construction sites.
John Hanley, Safety Officer at Mace said “the only way to deal with the problem was to introduce the right kind of deterrents so news of the clampdown would get around and bring any problems into the open. It is totally unacceptable that anyone high on substances should put fellow workers’ lives at risk.”. (Broughton, 2001)
According to Broughton (2001) anecdotal evidence is showing that on sites across the UK, drug use goes unchecked. It is hard to know how far the drug use culture is pervading the industry. Up to now, there has been no statistics from the Health and Safety Authority to link drug use to accidents. The majority of construction firms remain ignorant if the scale of the problem, but those who have observed the culture first hand must be tackled. (Broughton, 2001)
Alan Ritchie, a representative of the Union of Construction Allied Trades and Technicians (UCATT) in Glasgow says “When you think we have an ageing workforce that is going to be replaced by young people who could bring in a new drug culture, the industry will need to look at what measures need to be adopted to tackle [drugs].” (Broughton, 2001)Ritchie was involved in a case in which a member of UCATT alleged that drug use was taking place among construction workers on the £78m Millennium Wheel site in Falkirk, Scotland. Barry McDonald, a labourer on the job, claimed to have seen workers under the influence of cannabis and other substances. He even claims to have seen workers heat up marijuana in the canteen microwave. Morrison Construction, the main contractor on the job, launched an immediate investigation. A spokesman said “It must be remembered that the allegations are referring to probably only a couple or a handful of people from a site of 800 workers. Things needs to be kept in perspective.” Barry McDonald then left his job claiming intimidation from co-workers, “drugs are a big problem on building sites and people are making a real lot of money from dealing them.”(Broughton, 2001)
A graduate trainee working in London who did not want to be named says that “Saturday mornings are the worst……most of the team have been out on a Friday night and are still high on ecstasy, amphetamines and cocaine.” He says “I have recommended to lads whose pupils are still bulging from the night before that they go home because they are just not safe enough to operate machinery. You often get lads who are on something on site, whether it’s speed or some kind of pill taken to get them through the day. The problem is they often think they are Superman and try to jump from high places or lift a crane. They are the most dangerous.” (Broughton, 2001)
A labourer also from a site in London, who wished to remain anonymous, claims that he has also witnessed drug dealing on site. He believes it is something site managers are aware of and sometimes even overlook as it maintains worker morale. He says “There is one particular site in London where a lad has been dealing drugs for months. It’s not really done underhand; everybody knows he’s the man to contact to score drugs, and he knows he has a large marketplace to make money.” (Broughton, 2001)
Broughton (2001) writes that in November 1999, on site drug use hit national headlines when ecstasy and cannabis were reported being dealt during construction of the Millennium Dome. Employees of Northern Ireland-based firm Mivan were accused of dealing and taking drugs while working on two of the project’s 14 zones. Charlie Hutchinson, Mivan’s health and safety manager said “in our case the police didn’t want to know because the claims couldn’t be substantiated, but at the end of the day the contractor is liable and responsible for their employees.” Hutchinson believes that it is unfair that contractors are solely responsible for employees with sufficient powers to control and police them. He talks about sites in Florida in which drugs were eliminated from sites by random testing, “in the USA, drugs in the workplace are not tolerated. If we are to be responsible for employees, we too need some kind of powers to monitor workers, but here human rights legislation limits us from doing so.”
According to the International Labour Organisation (Drug and Alcohol Abuse Prevention, 2003) alcohol-related problems are more common in the work place than drug-related problems. O’Connor & Keenaghan (Alcohol and drugs in the workplace; attitiudes, policies and programmes in Ireland, 1993) state that Irish employers are of the opinion that absenteeism is the chief manifestation of alcohol abuse in the workplace. Studies carried out by Mangione, et al (Employee drinking practices and work performance, 1999), Bass, et al (Employee drug use, demographic characteristics, work reactions and absenteeism, 1996) & Normand, et al (An evaluation of pre-employment drug testing, 1996) have all shown the relationship between substance abuse and workplace absenteeism. There is also evidence available that shows a negative relationship between mixing drugs and alcohol and work performance (Lehman & Simpson, 1990) and that substance misuse is often associated with higher levels of injuries and accidents occurring at the workplace (Wells & MacDonald, 1999).
2.3.4 Forms of Substances and their effects
According to Designing Building (2017) “Construction projects, in particular, large and complex projects, are increasingly dependent on construction plant, and there are a wide range of issues that need to be considered in its use” including public and employee safety. Health and safety in particular is vitally important in the operation of plant on site particularly in regards to cranes, mobile plant and vehicles.
Hawkes Group state in their company drug and alcohol policy that “machine fitters/plant operators/lorry drivers/ground workers are requested to immediately report the use of any prescribed and/or over the counter medication that may have side effects while working whilst under the employment of Hawkes Plant Limited to the Management Systems Coordinator prior to embarking on the drugs.”
Hawkes Plant Limited will not accept any one to present themselves for work whilst under the influence of drugs or alcohol. Anyone is breach of this will be dealt with in accordance with the company’s disciplinary procedure. Hawkes Plant Limited’s machine fitters/plant operators/lorry drivers/ground workers must not:
- Report, or try to report, for duties when unfit for work through drugs or alcohol;
- Consume alcohol or drugs while on duty;
- Be in possession of alcohol or drugs on work premises;
- Drink 12hrs before or while on duty or take drugs at all;
- Wear high visibility or Hawkes Plant Limited identification or uniform on licensed premises;
- Use any drugs at any time;
- Have the smell of alcohol whilst on duty;
- Accept call for duty if in breach of any of the above or if they have any doubt about fitness to work. (Hawkes Group, 2016)
The following are different forms of drug that may have an effect on a plant and machine operator’s ability to drive or operate plant or machinery on site:
Alcohol
There have been studies that show that, in cases in which involvement in traffic accidents is concerned, no drug has been found to be as prevalent than that of alcohol. The majority of experimental studies have shown impairment on one or several performance skills at one or more BAC’s (blood alcohol content), with most impairments beginning at when the BAC is at or below 0.07g/dl (grams per decilitre). Experiments through simulators and on-the-road have typically shown alcohol to have deleterious effects on a number of driving skills including brake reaction time, ‘collision’ frequency, steering responsiveness and lane control, as well as the requisite cognitive skills such as risk-taking appreciation, planning and decision making. (Gemmell, Moran, Crowley, & Courtney, 1999)
Methadone
A series of studies have suggested that, in cases in which an individual has recently started using, the effect of acute methadone administration is to produce a dose-dependent reduction in reaction time, in visual function as well as information processing. In cases in which new patients on a maintenance program are concerned, literature suggests that it is recommended to allow a period of up to 30 days during which they should not drive. Like many drugs, methadone “can potentiate the deleterious effects of alcohol”. Both experimental and field studies suggest that methadone use does not result in significant driving impairments that deem the user ‘unfit’. (Gemmell, Moran, Crowley, & Courtney, 1999)
Cannabis
Although there is some conflicting evidence, it seems that cannabis does not significantly impair very basic perceptual mechanisms. However, cannabis does impair more subtle aspects of perceptual performance for example, attention and short-term memory, however these are most often seen in high doses. The majority of experimental studies have used low dose of cannabis and this may not reflect the does used by heavy marijuana users. Studies have demonstrated that cannabis is one of the most prevalent drugs discovered in the urine and blood samples of drivers. The assessment of the casual role of cannabis in accident occurrence us complicated by the fact that alcohol is most generally present in samples. When cannabis is mixed with alcohol, it is much more likely to be a risk factor than when consumed alone.
Benzodiazepines
The sedating effects of benzodiazepines can potentially cause some impairments on psychomotor tests. Studies have shown that benzodiazepines are the most frequently detected illicit drugs in all driver groups. Various authors have concluded that some benzodiazepine tranquillisers can impair driving skills throughout the first number of weeks of treatment, but these effects may deplete with continued use. Xanax and Valium are examples of a benzodiazepine. (Gemmell, Moran, Crowley, & Courtney, 1999)
Antihistamines
Experiments have suggested that peripherally active as opposed to centrally active antihistamines are less likely to cause any form of impairing sedative effects. Some forms of antihistamines are slow in crossing the blood brain barrier and therefore produce tolerance without central effects such and astemizole and terfendine, are more likely to have little detrimental effect on skill performance. Antihistamines vary in their effects on impairments and it is important that pharmacists, general practitioners, nurses and the general public are informed about the need of using the least sedating drugs that are available. Through studies, it is found that antihistamines are seldom suggested as causative factors in traffic accidents. Similar to cannabis, where antihistamine traces are found in fluid samples, alcohol is also presents in many cases. However, there is evidence to suggest that antihistamines potentiate alcohol effects. Generally, the use of peripherally acting antihistamines is not very likely to cause any impairments in driving performance. (Gemmell, Moran, Crowley, & Courtney, 1999)
Antidepressants
Investigations have suggested that antidepressants can have both positive and negative effects on psychomotor performance. Various studies have found that patient’s performance may improve as the result of the drugs relieving their depressive symptoms, however, more needs to be known about the effects of depression on the individual’s ability to drive. There is no clear picture from studies regarding the antidepressant levels responsible for traffic accidents compared to the overall driving population. There is insufficient research available on the newer, less sedative antidepressants regarding their effects on psychomotor performance. In the most popular antidepressants such as fluoxetine, the most common side effects sucg as nausea and insomnia can in itself effect driving. In situations where alcohol is combined with antidepressants, more so in the more sedative types, the worst impairments are often seen in the initial phase of treatment as diminish after treatment. Still, alcohol is the bigger problem and the effects of severe, untreated depression on driving capacities may be worse than the effects of antidepressants. (Gemmell, Moran, Crowley, & Courtney, 1999)
Amphetamines
Studies have shown that at lower risk doses amphetamines have little effects on cognitive functioning, however at higher doses risk-taking increases and responses are more inappropriate. Lower doses can result in an enhancement of various psychomotor tasks. There is insufficient evidence to specifically implicate amphetamine use in traffic accidents due to the lack of studies. Few studies have directly examined alcohol-amphetamine interactions and the results appear to be contradictory. Generally, high doses of amphetamine are likely to increase the impairing effects of alcohol, Therefore, there may be subjective positive stimulant effects associated with the use of amphetamines, although, these effects, more so at higher does could result in a change of personality leading to a more likelihood of impaired driving. (Gemmell, Moran, Crowley, & Courtney, 1999)
Ecstasy and Other Synthetic Drugs (GHB, Ketamine, PCP, Fentanyl, Ephedrine and Phentermine)
It is evident from comparatively inadequate literature on MDMA and various other synthetic drugs and driving that more research is needed in order to increase the understanding of the impairing effects of this drugs. Most research has concentrated on the short-term effects of MDMA but little is known of the consequences through use in the long-term. Ecstasy tablets are often made up of numerous, potentially toxic elements, the combined effects of which are mostly unknown. Likewise, there is very little evidence concerning the effects of GHB, ketamine, PCP, fentanyl and abused diet drugs on an individual’s driving abilities and in most field studies they are not detected often. Given the known side-effects of these drugs however and especially given the perception-changing effects of some. Notably PCP and fentanyl, it is likely that the establish a danger where driving is concerned. (Gemmell, Moran, Crowley, & Courtney, 1999)
2.4 Substance Abuse Related Workplace Accidents
According to Laad, et al (Prevalence of substance abuse among construction workers, 2013) the construction industry is among the largest economic activities of which plays a significant role in the nation’s economy. A lack of greater employment in various other sectors has drawn large numbers of workers to the construction industry in years before ‘The Crash’. Laad, et al (Prevalence of substance abuse among construction workers, 2013) notes that heavy physical work is required by workers in the construction industry while living in a run-down environment. The lack of recreational activity, company of friends, unhygienic situation encourages workers to take part in certain negative activities. Laad, et al (Prevalence of substance abuse among construction workers, 2013) repeats that substance abuse is often influenced by various factors including individual attitudes and beliefs, social norms and easy affordability. Often, workers believe that alcohol and tobacco use can benefit them in their work, however there are a lot of misconceptions. Cook, et al (The Prevention of Substance Abuse among Construction Workers: A Field Test of Social-Cognitive Programme, 2010) challenges the benefits that include helping the workers to suppress appetite, increase concentration, induce feeling of pleasure and reduce tension. Laad, et al (Prevalence of substance abuse among construction workers, 2013) reports that the construction industry makes up some of the highest rates of substance abuse, with the rate of current illicit drug use said to stand at around 14.1%.
The Government of South Australia (2006) believe that guidelines for addressing alcohol and other drugs in the workplace suggest that there is a necessity to identify hazards associated with the use of alcohol and other drugs in the workplace as well as the risk assessed and strategies developed to control the risk similar to any other occupational safety hazard. There needs to be consideration for a range of factors when assessing whether alcohol or drug use poses a health and safety risk within the workplace. Consideration towards the effect of drug intoxication and the hangover effects of drug must be made. Depending on the nature of the workplace the risk associated with alcohol and drug use may be greatly increased. Workers who operate machinery, drive or rely on construction or motor coordination may be at an increased risk of injury if affected by alcohol or other drugs. Workers who use heavy machinery or hazardous materials in their line of work, for example, may be at risk of more serious harm if injured.
The Government of South Australia (Guidelines for addressing alcohol and other drugs in the workplace, 2006) notes further that in some occupations, a worker whom is affected by alcohol of another form of drug may be more likely to place risk on the health and safety of others, for example, when moving hazardous materials or performing duties while part of a team. Alcohol and drug consumption may also be more prevalent in some industries than others. This is backed up by the U.S. Department of Labour who state:
“The major industry groups with the highest prevalence of heavy alcohol use was construction, arts, entertainment and recreation, and mining, and those with the lowest were healthcare and social assistance and educational services”.
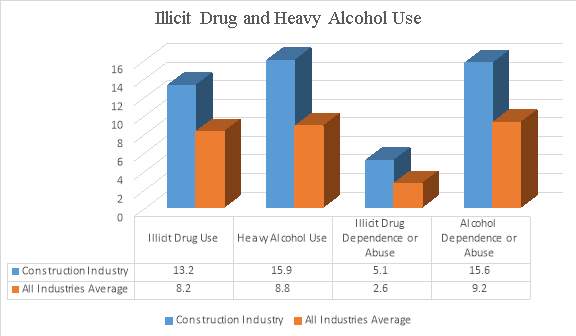
Figure 3 – Illicit Drug and Heavy Alcohol Use – U.S. Department of Labour
The above chart, provided by the U.S. Department of Labour highlights that heavy alcohol and illicit drug use as well as their dependence or abuse is more prevalent in the construction industry than the average of all other industries. Illicit drug use in the construction industry stands at 13.2% of those surveyed while the average of all other industries stands at 8.2%. Illicit drug dependence or abuse in the construction industry (5.1%) is nearly double that of the average of other industries (2.6%). Alcohol dependence or abuse proves to be more prevalent in construction (15.6%) than in other industries (9.2%).
An employer is required to minimize any risk caused by alcohol or other drug use in their workplace under their general duty of care to provide a safe working environment.
According to the work of Larson, et al (Worker Substance Use and Workplace Policies and Programs, 2007) three out of the five occupations with the highest prevalence of current illicit drug use were dominated by males. Larson, et al (Worker Substance Use and Workplace Policies and Programs, 2007) states that an estimated 97.4% of construction workers were male with similar figures showing in installation of maintenance and repair, and transportation and material moving at 96.2% and 87.2% respectively.
A survey carried out by Hogan, et al (Construction apprentices’ attitudes to workplace drug testing in Ireland, 2006) notes that 4.6% of the construction apprentices that were surveyed reported having an accident due to the use of alcohol while 3.6% reported to having an accident due to drug use. Hogan, et al (Construction apprentices’ attitudes to workplace drug testing in Ireland, 2006) further stated however, that if those percentages were applied to the total number of apprentices in the country (15,614 – construction apprentices) and if 4% of apprentices reported an accident due to the use of alcohol or other drugs, 625 people would suffer an accident in a year with alcohol or drug use contributing to the accident.
The researchers found that 40% of the respondents had reported feeling drunk in the year previous and 82.1% reported feeling hungover having consumed alcohol the previous night. As a result of drinking, 45.7% missed days from work, 70.7% felt tired at work and 62.9% left early or arrived late. Drug use, however, seems to impact less on work, with only 2.9% missing days from work and 9.3% leaving early or arriving late with only 10% feeling tired and 6.4% feeling hungover at work.
2.4.1 Reviews on Relationship between Substance Abuse and Misuse and Occupational Injuries
In 1993 and 1994, literature was reviewed with the aim of investigating the relationship between substance use and misuse and occupational injuries. In the first of the two reviews, Stallones & Kraus (The Occurrence and Epidemiologic Features of Alcohol Related Occupational Injuries, 1993) found that there was not enough evidence available to establish a relationship between alcohol use and misuse and workplace injuries. The Institute of Medicine (IOM) carried out their own review a year later on drugs and the American workforce (Normand, Lempert, & O’Brien, 1994). The IOM’s report conducted a more detailed review of the impact of alcohol and other drugs in the workplace and their outcomes including job satisfaction, absenteeism and accidents. The Committee concluded that while there was evidence that substance abuse effected job behavior and occupational outcomes including injury negatively, substance use’s influence on these injuries were small. However, the IOM’s study shows that there is a lack of analytical approaches to the study limiting their ability to say anything definite about a drug/accident relationship. Most available studies lacked controls for personality traits and other risk taking dispositions in multivariate models. Both Stallones & Kraus (The Occurrence and Epidemiologic Features of Alcohol Related Occupational Injuries, 1993) and IOM noted that very few studies employed a control group therefore limiting their ability to estimate differential risk between using and non-using groups.
2.4.2 Alcohol Use and Occupational Injuries
A number of different studies found wide, positive effects on self-reported alcohol use on occupational injuries. The relationship between alcohol use and work-related injuries was carried out by Stallones & Xiang (Alcohol consumption patterns and work related injuries among Colorado farm residents, 2003) among farm residents in Colorado between 1993 and 1995. The consumption of alcohol had a large effect on reporting a work-related injury. Those who drank alcohol three or more on average, had about 3.2 injuries per 10,000 person-work-days (c. 40-years’ work) compared to 1.9 injuries per 10,000 for those who do not drink alcohol, a 70% increase in risk. 3.2 injuries per 10,000 person-work-days is a yearly rate of 8 injuries per 100 workers. The rate for non-drinkers would be 4.8 injuries per 100 workers. Therefore, if 10 million workers are drinkers (from 140 million) there would be over 320,000 yearly injuries due to alcohol. Dawson (Heavy drinking and the risk of occupational injury, 1994) noted a positive relationship between drinking five or more drinks daily in the past twelve months and having a workplace injury among respondents in the 1998 National Health Interview Survey (Odds Ratio* – 1.74). (Shipp, Tortolero, Cooper, Baumler, & Weller, 2005) investigated the rates in the previous month (30 days) and self-reported injuries while working for income among secondary-school students in Texas. The research found a dramatic increase in risk between light users (OR* – 1.56) who drank 1-19 days in the last 30 days and heavy users (OR* – 10.55) who drank every day in the last 30 days.
Wells & MacDonald (The relationship between alcohol consumption patterns and car, work, sports and home accidents for different age groups, 1999) found through a telephone survey in Canada that increased drinking was associated with a larger number of self-reported accidents among 15-24 year olds but not for older groups. However, those that drank more than 14 times a week were more than likely to report having an accident at work. Mangione, et al (Employee drinking practices and work performance, 1999) found that very light- moderate drinkers reported half as many injuries to that of heavy drinkers. However, these positive results were balanced by studies that used self-reports and found no effects of alcohol and injury at work. Ames, et al (The relationship of drinking and hangovers to workplace problems, 1997) found no effect of any of their measures of drinking behaviour on workplace injuries on a group of manufacturing workers. However, they did note a significant effect of drinking and other problems in the workplace i.e. disputes with colleagues and sleeping at work. Hoffman & Larison (Drug use, workplace accidents and employee turnover, 1999) as well as Veazie & Smith (Heavy drinking, alcohol dependence and injuries at work among young workers in the United States labour force, 2000) also found little reason to conclude a positive relationship between drinking alcohol and injury in the workplace.
| Source | Sample | Measure of Substance Use | Injury | Findings |
| (Dawson, 1994) | 29,192 adults interviewed in National Health Interview Survey 1988 | Self-Report – Use of Alcohol (≥5 drinks over number of days in last year. | Self-Report – Injury at work in last year. | Frequent and less frequent heavy drinkers were more likely to report an on-the-job-injury. |
| (Ames, Grube, & Moore, 1997) | 832 hourly employees in a U.S. manufacturing plant over 5 years | Self-Report – Use of Alcohol (before, during and after work and working when hungover). | Self-Report – Injury at work in last year. | Alcohol was not associated with injury but was associated with sleeping at work and fighting with co-workers. |
| (Hoffman & Larison, 1999) | 9,097 workers in National Household Survey on Drug Abuse 1994 | Self-Report – Use of Alcohol over the last year. | Self-Report – Injury at work in last year. | No association was found between alcohol and work related accidents. |
| (Mangione, et al., 1999) | 6,549 employees from 6 sites, 1994 | Self-Report – Use of Alcohol. | Self-Report – Injury at work in last year. | There is a relationship between alcohol use and injuries with heavy drinkers having the highest injury rate. |
| (Wells & MacDonald, 1999) | 10,385 Canadians (15+) | Self-Report – Use of Alcohol (quantity and frequency in past week and 12 months). | Self-Report – at least one work accident in last year. | Heavy drinking was associated with self-report of having at least one accident in last 12 months. |
| (Veazie & Smith, 2000) | 8,569 in National Longitudinal Survey of Youth (24-32) | Self-Report – Use of Alcohol (quantity and frequency currently, dependence). | Self-Report – Injury (exc. Strains and sprains) in past 6 months at work. | No link was found between work related accidents and alcohol consumption. |
| (Stallones & Xiang, Alcohol consumption patterns and work related injuries among Colorado farm residents, 2003) | 872 farm residents in Colorado | Self-Report – Use of Alcohol (quantity and frequency in past week and month). | Self-Report – Injury at work in last year. | Farmers who drank more often had higher injury-incidence rates. |
| (Shipp, Tortolero, Cooper, Baumler, & Weller, 2005) | 3,365 high-school students in South Texas, 1995 | Self-Report – Use of Alcohol and Drugs over the past 30 days (alcohol and cannabis), lifetime use (cocaine, inhalant and steroids). | Self-Report – Injury while working for income – lifetime. | Risk of injury increased for all substances with higher rates of current and lifetime use. |
Figure 4 – Findings of other researchers on alcohol use and occupational injuries
* An odds ratio (OR) is a measure of association between an exposure and an outcome. The OR represents the odds that an outcome will occur given a particular exposure, compared to the odds of the outcome occurring in the absence of that exposure
2.4.3 Drug Use and Occupational Injuries
Hoffman & Larison (Drug use, workplace accidents and employee turnover, 1999) also examined the impact of drug use on occupational injuries during their analysis of the 1994 National Household Survey on Drug Abuse. They found no evidence of a relationship between drug use (cannabis and cocaine) and occupational injuries. However, this finding is different to the findings of three other studies who all found significant evidence of positive relationships between self-reports of the use of drugs and occupational injuries. Shipp, et al (Substance use and occupational injuries among high school students in South Texas, 2005) looked at the frequency of alcohol consumption, binge drinking and cannabis usage over the past month as well as lifetime usage of cannabis, cocaine, inhalant and steroids. The study consisted of 3,365 Texan high-schoolers who were currently working. The study found that there was an increase in the odds of reporting an injury if there was an increase in the frequency of substance use. Frone (Predictors of work injuries among employed adolescents, 1998) also studied high-school aged workers and found that self-reported on-the-job substance use had a high positive effect on the chances of an injury occurring. However, he did not find a relationship between general substance use and injury. Kaestner & Grossman (The Effect of Drug Use on Workplace Accidents, 1998) found that the use of cannabis and cocaine in the past year increased the chances of reporting a workplace accident over a year by 25% in men, however, there was no evidence of a relationship among women.
2.5 Employer’s and Employee’s duties in relation to drug use in Ireland
2.5.1 Employer’s and Employee’s duties
There is no requirement for a worker to undergo testing for intoxicants under current health and safety legislation. Similarly, employers do not have a legal obligation to test their employees for intoxicants. As previously mentioned in the introduction there is a clause 13(1)(c) in the (Health and Safety Authority, 2005) Safety, Health and Welfare at Work Act 2005 (the Act) which allows for regulations to be made for intoxicant testing. However, this clause does not apply today until the regulation is introduced by the relevant Minister.
The Act defines intoxicant as alcohol and drugs and any combination of drugs and alcohol. It includes both legal and illegal substances meaning over-the-counter and prescribed medications are included.
The relevant duties of the employer are set out in Section 8 of the Act (Health and Safety Authority, 2005). These duties require the employer to ensure, so far as reasonably practical, the safety, health and welfare of all his or her employees. This includes managing and conducting work activities to prevent improper conduct or behaviour that will likely put employees at risk. Section 19 (Safety, Health and Welfare at Work Act 2005, Section 19, 2005) and 20 (Safety, Health and Welfare at Work Act 2005, Section 20, 2005) of the Act state that employers must identify hazards in the workplace; to have a written assessment of the risks as a result if those hazards in the workplace, the safety statement should state it.
While at work, an employee must ensure that he or she is not under the influence of an intoxicant in which they could endanger themselves or the other people present at the time, Section 13(1)(b). The employee must also fully co-operate with their employer to comply with health and safety law e.g. an employer should inform their employer if they are taking any medication that may pose a risk to other workers.
Where intoxicants at work is identified as a hazard it must be entered within the safety statement of the company. Although there is no requirement for testing of employees, employers should address whether the employee’s behaviour poses a risk of danger to himself/herself or others. The correct course of action would be to remove the employee from the situation if it is the case. Where testing is part of the company policy or has been put into their employee’s contract, it is recommended that tests are carried out in accordance with a recognised standard i.e. European Laboratory Guidelines for Legally Defensible Workplace Drug Testing.
2.5.2 Disciplinary Procedure
Other than any enforcement action by the Health and Safety Authority in regards to breach of employee duties, any employee who does not adhere to requirements of statutory regulations and/or site safety rules may be liable to disciplinary action. This could be the employer’s disciplinary procedures up to and including dismissal.
Breaching any safety procedure is a very serious matter with some breaches a lot more serious than others and may warrant summary dismissal. Among the many breaches of safety breaches, reporting for work whilst under the influence of alcohol or drugs is one of the more serious of breaches. This would be considered an act of gross misconduct warranting summary dismissal. Any allegations would be investigated thoroughly and would comply with natural justice. (Construction Industry Federation, 2003)
2.6 Remedies and Actions of preventing Substance Abuse in the workplace
2.6.1 Treatment Recommendations
By reducing employee substance abuse employers can decrease health care costs, reduce injuries in the workplace and improve productivity. Like asthma and diabetes, there is an understanding that substance addictions are chronic addictions.
Similar to these chronic conditions, addiction to substances can be managed successfully. However, it is not uncommon for a person to relapse or in terms of substance addiction, begin to abuse substances again. Relapse does not mean failure; it simply means that treatment is necessary again or a different form of treatment is required. (U.S. Department of Health and Human Services, 2007)
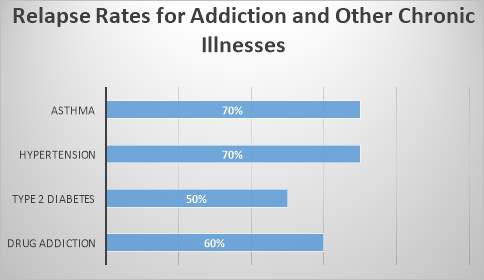
Figure 5 – Relapse Rates for Addiction and Other Chronic Illnesses – (McLellan, Lewis, O’Brien, & Kleber, 2000)
Identifying Substance abuse early can save employers and companies money in terms of health and productivity costs. An employer substance abuse programme may include workplace policies, drug testing, employee educational promotion, employee assistance programmes (EAP’s) and health plan treatment coverage.
A complete employer substance abuse programme shall include:
- Confidential screening by an EAP or health professional.
- A workplace substance abuse education component.
- Treatment referrals to an EAP or health professional.
- Confidential follow up care for supporting any employees in recovery.
2.6.2 Workplace Policies and Drug Testing
A substance abuse policy may implement a drug-free workplace initiative. A complete substance abuse policy might include: (Canadian Centre for Occupational Health and Safety, 2005).
- Purpose and objectives of the policy;
- A definition for substance abuse;
- Who is covered by the policy;
- Under what conditions will drug testing (inc. alcohol) be conducted;
- Confidentiality rights of the employee;
- Educational opportunities regarding substance abuse for employees e.g. substance-free awareness programme;
- Training for employees for identifying impaired behaviour and other signs of substance abuse;
- Guidance on how to deal with impaired workers;
- Provisions for supporting and helping chronic substance abuse;
- Disciplinary actions.
Some industries have specific legal obligations to address workplace substance abuse. For example, employers in transportation must ensure the safety of their employees and the public travelling on their mode of transportation.
It is essential that companies or employers are completely aware of patient/employee substance abuse confidentiality rules. Federal regulations regarding the confidentiality of patient’s records of drug and alcohol use have been issued by the Department of Health and Human Services. Employers must emphasise with the assurance their privacy will be protected.
2.6.3 Employee Assistance Programmes (EAP)
Employee Assistance Programme (EAP) access is offered to employees by the majority of large employers. The EAP have expertise in providing information, referrals and counselling on issues such as substance use, stress, family problems, mental health and work. The EAPs guide employers in addressing various employee problems and proactively deal with workplace issues that may lead to violence, declining morale and physical and mental health issues. The programmes are staffed by professionals who provide the individuals and their families with prevention services and short term problem-resolution services. The EAPs provide, what could be very helpful in the construction industry, confidential substance screening, education, recovery support and referrals for treatment. Other than the health benefits the programmes offer, they play a major role in encouraging employee wellness while reducing substance abuse among various other health problems. (Employee Assistance Professionals Association, 2017).
2.6.4 Health Plans
National Business Group on Health (An Emplyer’s Guide To Workplace Substance Abuse, 2009) highlight that health plans should provide coverage for substance abuse screening, therapy, counselling and aftercare. By offering a comprehensive health plan with benefits, employers can help make treatment successful. A broad range of services the plan supports are:
- Confidential substance abuse screening;
- Brief intervention;
- Outpatient and inpatient treatment;
- Medication;
- Peer support groups;
- Illness self-management programmes;
- Counselling and medical services;
- Follow-up services during treatment and recovery.
2.6.5 Workplace Health and Wellness Programmes
An employer can play a major role in preventing the hazardous use of legal and illegal substances by:
- Making it clear that drinking and the use of illicit drugs on site is not condoned;
- Combating the stigma workers have against looking for help and promoting that employees can seek treatment confidentially without jeopardizing their jobs;
- Stating information of the appropriate use of alcohol and various legal substances such as prescribed medication and over-the-counter medication into a wellness and risk prevention strategy;
- Provide factual information to employees on the harmful effects alcohol and drug use has on them;
- Informing employees of the health and safety risk excessive or binge drinking outside of work has.
(Human Resources Council, 2017)
2.6.6 Treatment
The Center for Substance Abuse Treatment (CSAT) define treatment as “in-or-out-patient services that focus on initiating and maintaining an individual’s recovery from alcohol or drug abuse and on preventing relapse.”
A large number of individuals with a substance abuse disorder do not receive the care they require. Mark, et al (Spending on mental health and substance abuse treatment, 1987-1997, 2000) found that 47% of men and 41% of women in need of drug use treatment are not treated. The strongest argument for the use of the solutions that this dissertation has to offer is the opportunity to reduce the monumental costs in terms of health, disability and liability that companies experience due to undiagnosed and untreated substance abuse. As shown in Fig.10, treatment for substance abuse is just as successful as treatment for asthma, diabetes and other chronic diseases. Previous studies have shown that up to 70% of patients treated for substance dependence recover. (American Psychiatric Association, 2000)
Those who seek and receive treatment for their addictions have:
- Better long-term outcomes;
- Improved long-term health;
- Reduced relapse;
- Improved family and other relationships. (U.S. Department of Health & Human Services, 2002)
2.6.7 Screening and Assessment
Screening is carried out in order to determine whether or not an individual shows any clear indicators of substance abuse. The answer is simply yes or no. The process attempts to quickly identify potential or current substance abusers so that appropriate interventions can be provided. There are many ways in which screening can be done including in the workplace, at home, online or in a physician’s office. In many cases screening may be the first recovery step. (National Center for Biotechnology Information, 2017)
According to O’Connell (A systematic review of the utility of self-report alcohol screening instruments in the elderly, 2004) the CAGE was the most widely used screening tool followed by Michigan Alcoholism Screening Test (MAST) and Alcohol Use Disorders Identification Test (AUDIT). They found that the newer instrument, the AUDIT-5 is showing some promising results. The Substance Abuse Subtle Screening Inventory (SASSI) is used to identify alcohol and drug abusers and differentiate them from social drinkers etc.
Assessment is a process for defining the nature of that problem, determining a diagnosis, and developing specific treatment recommendations for addressing the problem or diagnosis. (National Center for Biotechnology Information, 2017)
2.7 Case Study
2.7.1 ‘Spotlight On’ Scheme
Throughout the Construction Industry in the UK, alcohol and drugs have been recently placed under the Considerate Constructors Scheme after the results of a survey revealed that 59% of people working within the industry are concerned over the effects drugs and alcohol have on the industry.
The ‘Spotlight On’ campaign scheme focuses on taking the various measures necessary to protect and safeguard the entirety of the workforce in relation to drugs and alcohol.
A survey recently carried out with over 1300 people working in the industry discovered that 59% have concerns over the effects of drug and alcohol in construction and yet 65% have never been tested for either alcohol or drugs.
The survey, which was conducted by the Considerate Constructors Scheme in May of 2016 also revealed:
- 39% admitted the issue of drugs and alcohol could be better tackled in their workplace;
- 35% have noticed their co-workers under the influence of drugs and alcohol;
- 25% agreed drugs and alcohol affected them at work through tiredness;
- 23% agreed it affected them through decreased attention during work;
- 19% agreed the effects made them less productive at work.
Many contractors as well as suppliers and clients of the construction industry undertake ‘rigorous and regular measures’ to tackle the issue which includes zero tolerance to alcohol and any form of drug, random testing, providing information regarding drugs and alcohol through toolbox talks, site inductions and resources such as posters around the site.
(Safety & Health Practitioner, 2016)
A number of Scheme-registered contractors have provided case studies on how they tackle this issue, including: John Sisk & Son Ltd, Ballymore and Mulally and Co Ltd.
Case Study: John Sisk & Son Ltd
Sisk have a Substance Abuse policy which they implement across all their jobs. Below is an extract from their policy:
“The law imposes obligations to provide a safe system of work. In addition, it also requires employees to take reasonable care of their own safety and also that of their colleagues. The possession, use or supply of drugs and alcohol is strictly prohibited…
…Where the company suspects that you have consumed drugs or alcohol…[it can]…request that you attend…an examination…In addition the company undertake random tests…”
In the UK, random testing is allowed and can take place at any time. In Ireland, the Safety, Health and Welfare at Work 2005 Act Section 13(c) clause is a very grey in the sense that it is there to be done but difficult to enforce unless clear stipulated in the employee’s contract.
Sisk implemented the procedure on the Temple Quay, Phase 3 project in order to prevent personnel being on site while under the influence of drugs and/or alcohol.
All personnel were informed, as part of the induction to site, of the company’s Substance Abuse policy and informed them that random drug and alcohol testing would be carried out every six weeks during the project. Two personnel from site would be randomly selected and taken to a clinic where they would be tested, with the target being to test 5% of the workforce every six weeks. As the site was small, it wasn’t feasible to have a full time testing facility on site.
The Site Manager confidentially arranged the test date and two appointments were booked into the clinic. All site personnel including management, sub-contractors and agency personnel names were included and two names were selected at random. Those chosen were taken to a clinic by a member of site management and accompanied at all times.
An alcohol test (breathalyzer) was carried out and a urine test was also carried out for a definitive alcohol and drugs assessment.
Test results were reviewed after they were issued and if levels reported were above the threshold value, the individual concerned would be instructed to stop working and leave site immediately. All individuals were given a copy of their test report.
Additionally, Sisk site management continually observed personnel for any drug and alcohol abuse symptoms throughout the project and if they suspected abuse they were sent for testing.
Toolbox talks were given throughout the course of the project to remind personnel that they must not be on site if under the influence of drugs and/or alcohol. (Considerate Constructors Scheme, 2016)
Case Study: Ballymore
In order to help raise standard on-site, Ballymore put together a series of health and safety awareness features. The London City Island Project is a great example of a project the which a coordinated effort to tackle the alcohol and drugs issue by keeping the topic on employee’s minds by means of visual aids. The implementation of on-site testing and easily accessible support systems shows that the company is committed to a direct action approach to the situation.
The company’s drug and alcohol policy includes a clear annual and random testing regime of nothing less than 20% of the workforce. Guidance and support systems will be offered if an individual states their drug or alcohol problem before being testing, encouraging an attitude of seeking help. Similarly, anyone refusing a test shall face disciplinary actions.
Drug and alcohol toolbox talks have been constructed with a designed approach to educate the workforce on the important information on drug and alcohol use. The site has incorporated resources from the health and wellbeing service; Compass, along with information of their own. Included in the presentation is the following:
- Drugs and alcohol statistics;
- Definitions and examples of each drugs class;
- Consequences of being convicted for each drug class;
- The effects and impacts of being addicted to drugs;
- The effects and impacts of being addicted to alcohol.
Providing a greater and more contextual understanding to drugs and alcohol gives individuals the knowledge to make better decisions, avoiding what can be life changing and leading them down a dangerous path. FRANK is a contact source for drug support and advice service.
As well as advertising a direct advice centre through toolbox talks, the site has also implemented an alternate means for support. A site phone has been provided for anyone who does not feel comfortable expressing themselves to the site’s own advisors. Details of Construction Industry Helpline are provided that also serve as a support and advice centre for various concerns including drugs and alcohol.
Visual reminders have been incorporated onto site through ‘Here is my reason. What is yours? posters that focus in being safety conscious.
The posters serve as a way of portraying why it’s important to stay alert and maintain safety, with a thoughtful reason in mind. Although this is not solely associated with the risks of drugs and alcohol, it emphasizes health and wellbeing on site, demonstrating a caring and proactive culture.

Ballymore have implemented a number of means to raise the awareness of drugs and alcohol on-site at the London City Island Project as well as offer channels of support that are easily accessible. The project demonstrates a great example of how easy it can be to introduce direct and effective features to site health and safety plans. (Considerate Constructors Scheme, 2016)
Case Study: Mulalley & Company Limited
Mulalley see the misuse of drugs and alcohol as a serious health and safety concern and like various other companies in the industry, their approach to tackling this is firm and direct. Mulalley has a zero tolerance drugs and alcohol policy for employees and also employees of any companies working on their sites or facilities.
The policy is clear in its approach to all substances from over-the-counter prescription medications to illegal drugs, all holding equal weight and strict consequences. Although the drink-drive limit is 80 milligrammes of alcohol per 100 millilitres of blood, the limit at Mulalleys is strictly zero.
Mulalley understand that if any substance is expected to or presents a possibility of physically and/or mentally affecting an employee’s ability to perform can cause a risk to health and safety. An individual must inform their employer of any over-the-counter medication so it can be assessed whether or not they’re fit to work.
Should an employee be involved in an accident at work or appears to be unfit through suspected alcohol or drugs use, they may be ordered to a drugs and alcohol test by approved external testing organisation. Raising and maintaining awareness of the company policy at site induction with toolbox talks and posters on site is a constant reminder of why the workforce should be considering their commitment to their own health and safety and other’s.
Mulalley has FORS (Fleet Operator Recognition Scheme) Silver accreditation and as part of this all Mulalley company van drivers undertake FORS online training including “work related road safety” which specifically discusses the risks and dangers of driving under the influence of alcohol and drugs.
Although testing is taken seriously with disciplinary action if necessary, Mulalley maintain a distinct approach of encouraging any employee who may be under the influence or having difficulties or problems to come forward. Identifying and communication the concern is the correct way to secure a positive and remedial solution. Like Ballymore, employees can contact the confidential Construction Industry Helpline for advice on addiction-related illnesses. (Considerate Constructors Scheme, 2016)
Chapter 3: Methodology
3.1 Introduction
In this section the researcher explains how the information is gathered through both the primary and secondary methods of research. Rajasekar, et al (Research Methodology, 2013) defines research methods as the various procedures, schemes and algorithms used in research. Rajasekar, et al (Research Methodology, 2013) also defines research methodology as a “systematic way to solve a problem” or the “science of studying how research is to be carried out”. In other words, research methodology is “the procedures by which researchers go about their work of describing, explaining and predicting phenomena.”
A methodology is essentially a central process in which various information is gathered and analysed later so that the researcher can reach a given conclusion before making appropriate recommendations. The researcher uses a series of methods in order to gain the necessary knowledge in substance abuse in the Irish construction industry. The researcher’s aim is to examine whether or not substance abuse is prevalent on Irish construction sites through research and analysis of feedback from contractors both large and small who may have experienced employees using alcohol or other illicit drugs on sites they have worked on.
In the literature review, the researcher gathered relevant information in relation to the topic through secondary methods of research from books, articles in journals, websites, newspapers and industry published works. This research was carried out to gain a better understanding of the topic, before conducting the primary research. The primary research will be qualitative mixed methodology in nature through surveys and semi-structured interviews with a number of contractors whom may or may not have experienced substance use on their sites.
3.1.1 Aim of research
The aim of the dissertation is to investigate and examine substance abuse and its presence in the Irish Construction Industry.
3.1.2 Research objectives
- Investigate drug abuse in Ireland and the Construction Industry.
- Examine the substances most commonly associated with workplace related accidents.
- Detail the Employer’s position and legal duties in relation to substance abuse on Irish construction sites.
- Investigate and propose possible remedies/actions that can be taken to combat substance abuse on construction sites in Ireland.
In a research project, it is important to choose the most suitable research methods. These methods play a vital role in validating the research topic. In order to complete, an accurate and completed account of information the researcher took a detailed look into the various types of research methods that are available and realistically achievable. From the research of such methods, the information established that research falls into two main categories. These are:
- Primary research
- Secondary research
The methods of research used in a research project are solely dependent upon the information required to prove or disprove the hypothesis. As a result, it is necessary to establish what information is needed before concluding on the methods to be used.
- An overview of general drug use in Ireland and the construction industry;
- Information regarding the substances that may affect construction workers operating machinery etc;
- An overview of the employer’s legal duties in relation to substance abuse on Irish construction sites;
- An examination of remedies that may combat drug abuse on construction sites.
3.2 Research Strategy
Naoum (Dissertation Research & Writing for Construction Students, 2007) believes that deciding on which type of research to pursue, depends on the research topic and the information available that is required to successfully complete the thesis. Research strategy can be described as the way in which the objectives of the research can be questioned. There are two types of research strategy, they are ‘qualitative research’ and ‘quantitative research’. For the purpose of this thesis, the researcher will use qualitative research to examine whether or not substance abuse is prevalent in the Irish construction industry.
3.3 Primary Research
Naoum (Dissertation Research & Writing for Construction Students, 2007) describes qualitative research as ‘subjective’ in nature with an emphasis on meanings, experiences often verbally described, descriptions etc. The information gathered can be classified under two categories, exploratory or attitudinal. Zikmund (Business Research Methods, 2013) states that researchers use exploratory for three interlinked purposes; diagnosing a situation, screening alternatives and to discover new ideas. Attitudinal is used to ‘subjectively’ evaluate the ‘opinion’, ‘view’ or the ‘perception’ of a person toward a particular ‘object’ often referred to as an ‘attribute’, a ‘variable’ a ‘factor’ or a question.
Primary research was carried out to obtain the rest of the information that was going to be used to test the hypothesis. Following research into possible research methods the researcher gathered from Naoum (Dissertation Research & Writing for Construction Students, 2007) and Zikmund (Business Research Methods, 2013) as well as the information gathered from the secondary research the author decided that one to one semi structured interviews would be the most appropriate.
Oppenheim says (2000) “interviews come into their own when we need to ask numerous open-ended questions, or open-ended probes, where the interviewer has to record verbatim the answers given by the respondents.”.
There are three types of interviews structured, semi-structured and unstructured. Structured interviews are made up of a predetermined set of questions that can be easily analysed. Semi-structured interviews are detailed as a framework for the actual topic. They are slightly more difficult to analyse however, there are no set of predetermined questions that will give the researcher a more in depth response allowing more information to be gathered. Naoum (Dissertation Research & Writing for Construction Students, 2007) describes semi-structured interviews a ‘more formal’ than the unstructured interview in the sense that there are a number of specific topics around which to construct the interview. This form of interview uses both ‘open’ and ‘closed-ended’ questions.
3.2.1 Research design
One to one interviews were conducted with members of two large main contractor and Salus. Throughout this research study, the prevalence issue relating to substance abuse was investigated. Further to this, a focus group was conducted with three individuals from a sub-contractor company based in Dublin.
3.2.2 Ethical considerations
The ethical principles governing this research were informed consent, anonymity, voluntary participation and freedom to withdraw.
Prior to each interview, total confidentiality and anonymity was explained to each participant. Participants were informed that they were free to withdraw at any time and the researcher answered all questions the interviewee had about the study. Bowling (2014) states that “this voluntary consent safeguards the freedom of the participant to choose to participate in the research or not, and reduces the legal liability of the researcher”. Permission was sought for the use of a tape recorder before conducting the survey. The researcher also explained to the participants the purpose for using the tape recorder, the tapes would not be listened to by anyone else other than the researcher and that it would be deleted after this thesis had been completed.
3.2.3 Sample Frame
Participants were health and safety officers with many years of experience behind them and members of a training services organization that provide health and safety training in diverse sectors. Those in the focus group were ground workers currently in the early stages of a project. Purposeful sampling was employed in this study. Participants were recruited from known, easily accessible populations. Bowling (2014) has highlighted that purposeful sampling has the advantages of ease of recruitment, easier monitoring and follow-up, generally good response rates and retention of sample members.
3.2.4 Sample size and Sampling strategies
Sampling is a major problem for any research. The selection criteria for the one to one interviews were that participants had to have relatively good experience and insight into construction health and safety, company drug and alcohol policies and a good understanding of health and safety law in Ireland.
3.4 Secondary Research
“The data collected using the desk study approach are called ‘secondary’ data because the data are obtained from other sources. Secondary data can be stored either in a statistical or descriptive format.” (Naoum, 2007)
In order to obtain information into the background of the subject area, secondary research was carried out. Research was undertaken in the form of a comprehensive literature review.
The review proved to be a helpful source of background information. The literature review was assembled from several areas such as:
- Contractor Drug and Alcohol Policies;
- Current Legislation;
- Academic Journals (SAGE, ResearchGate);
- Governing body websites (HSA);
- Databases (info4education)
- Textbooks, Trade journals.
Search engines such as Google and Google Scholar were also used to complete the literature review.
3.5 Interviewees
Interviewee 1
Interviewee 1 is a health and safety officer for a large main contractor based in Dublin. He has been an employee for the company for the last 16 years. This individual preferred to keep his own name as well as his company name anonymous.
Interviewee 2
Interviewee 2 is the HSEQ manager of the same company in which Interviewee 1 works. He has worked within the industry for the last 12 years. Interviewee 2 also wished to remain anonymous for the purpose of this thesis.
Interviewee 3
Interviewee 3 is Tom Sweeney, a health and safety officer for a different large main contractor based in a number of different countries. He has worked within the industry the past 12 years. Tom agreed to use his name but asked that the name of the company he works for to remain anonymous.
Interviewee 4
Interviewee 4 in Tom Browne, owner of Salus training services, a service that aim to provide a wide variety of health and safety training courses in a number of diverse sectors. Tom has worked within the industry for a long number of years. Tom agreed to allow his name as well as his company name to be used in this thesis.
Interviewee 5
Interviewee 5 currently works as a health and safety officer for the same company Interviewee 1 and 2 work for. She has worked in the industry the last 8 years. She too ask to keep her name and company name anonymous.
3.5.1 Access
All interviewees that participated in the research were contacted via email or telephone. The purpose of the study was explained and fortunately, many industry professionals agreed to participate. Time and dates were arranged with all participants.
3.5.2 The Settings
Each participant obliged to facilitate the interview either in their office at company headquarters or on site. This was a major advantage as a majority of the participants were easily accessible. Participants were familiar with the location and the surroundings, which is important in creating a comfortable atmosphere (Krueger, 2015).
3.6 Data collection
Made up of the following:
3.6.1 Procedure
Interviews:
Five interviews took place and well as a focus group made up of three employees on a project in Dublin. An office room was provided by each of the participants. This had the advantage that participants were familiar and comfortable with their surroundings. Also, all participants were obliging and welcomed the research. As discussed in the initial telephone call or email, the duration time was given again to assure the participant on his freedom to withdraw if needed. An introduction to the purpose of the study was again given and every effort was made to make sure all participants felt relaxed. An open ended questions approach was undertaken.
Each interview lasted for roughly 10-20 minutes. Once the interviews finished, the researcher gave feedback and highlighted the key points made by the interviewee. All notes were collected and tapes listened to.
3.6.2 Pilot study
A pilot interview was carried out to familiarise the researcher with the interview format and process and to identify any difficulties that might arise in the study by submitting the interview questions to the thesis supervisor and another college lecturer. This pilot study proved to the researcher that;
- The length of the interview was reasonable;
- The questions did not appear to be too intrusive;
- Terminology was appropriate.
3.6.3 Reflection on study process
On the day prior to one of the interviews, one of the participants broke their foot on site. This could not be avoided and fortunately did not interrupt the data that was gathered as the interview was set at a later date. Before each interview commenced, the researcher had a conversation about the college course as well as the current state of the Irish construction industry to bond with the participants. This made the participants relax and feel at ease with the research process.
Most participants identified their experiences if any of substance abuse on sites on which they worked and their opinions of current legislation in regards to drug testing etc. The researcher presented himself as a student and participants acknowledged this and tried to answer questions to the best of their ability. All interviews ran freely and smoothly and the researcher felt that, as the interviews went on most participants enjoyed them and didn’t mind if the duration of the interview exceeded the stated duration at the start.
3.7 Data analysis
Yin (2014) describes data analysis as consisting of examining, categorizing, tabulating, or otherwise recombining the evidence, to address the initial propositions of the study.
The interviews were analysed separately after the data collection was completed. The recorded interviews were transcribed verbatim. The researcher employed the following method.
All interview texts were read and re-read while listening to the recording. The researcher made written comments and observations throughout the interviews. These were all included. Once an understanding of the whole text was obtained, thematic analysis began. The text was again read sentence by sentence and themes and sub-themes were highlighted and underlined. Additional comments were written on the margin of all texts. The researchers then cut and paste the data to develop emerging themes. These emerging themes gave the researcher an insight into the prevalence of substance abuse on Irish construction sites.
Chapter 4: Analysis of Data and Findings
4.1 Introduction
The main aim of this study is to investigate and examine substance abuse, its presence and affects in the Irish Construction Industry. The methodology that was employed was qualitative data collection through the use of interviews and a focus group.
The following are findings from the qualitative data.
4.2 Qualitative Findings
In order to best present these findings, certain abbreviations have been made. The letter P stands for Participant, and the numbers 1-5 relate to the interviewee code number found in Chapter 3. For example, one of the participants will be known as P1 and so on and the four participants in the focus group will be known as FG1 through FG3.
From analysing the qualitative data, certain themes emerged. These themes will be presented under the following headings:
- Past and Present;
- Suspicions of substance abuse on site and resulting accidents;
- Link between accidents and alcohol/illicit drugs;
- Flaws in Safety, Health and Welfare at Work Act 2005;
- Lack of drug testing conditions in contracts;
- Substance use course of action;
- Workplace policies;
- Future problem;
- Introduction of random drug testing in Ireland
4.2.1 Past and Present
All participants were probed on whether they believe that substance abuse is prevalent on construction sites in Ireland at present or even in the past. The first construction professional interviewed of Company A (P1) stated that
“I would say at present no, I don’t think it’s that common at the moment, in the past possibly, 10 or 11 years ago when things were really moving, when business was very good, people had a lot more disposable income then. Not as prevalent at the moment.”
The HSEQ manager (P2) of the same company was of a similar belief with his statement
“Substance abuse is not that prevalent on sites here at present. In the past you would get a strong smell of booze from a large enough cohort on a Monday morning but this is quite rare nowadays, so much so that you easily notice when someone is hungover. Drugs are a little harder to spot but I would say that the smoking of cannabis and hash is common enough in places.”
Tom Sweeney (P3), a health and safety officer for Company B pointed out that he “thinks alcohol and drug use is prevalent currently” on construction sites in Ireland while Tom Browne (P4), owner of Salus Training Services believes it “exists but is not prevalent”. P5 who is also currently employed as a health and safety officer for company A is absolutely convinced that substance abuse is prevalent on Irish construction sites stating “yes, substance abuse is definitely prevalent on construction sites in Ireland both past and present.”
The focus group was made up of three employees of Company C, more or less believe it was more prevalent in the past but still think it exists today.
FG1 stated that “I have worked on site in both Ireland and in the UK for the last 15 years and I believe it is a problem but more so in the past.” FG2 who has lived in Ireland the last five years said that “I have not seen too much of it since I came to work here but there have been one or two occasions involving alcohol” while FG3 was in agreeance with FG1, “Like [P1] said, I believe it does happen today but more of a thing of the past, I think money is a factor. Maybe with the lack of worker in the past number of years we simply haven’t seen it.”
4.2.2 Suspicions of Substance Abuse on Site and Resulting Accidents
Regarding their own personal suspicions of workers consuming alcohol or using drugs on site, all participants admitted their suspicions.
One of the interviewees spoke about “one occasion 11 years ago, we dealt with it very sensibly. One occasion in 14 years for me. We were given a heads up that someone was seen consuming alcohol not too far away from the site and it was dealt with off-site.” (P1)
Tom Sweeney (P3) who worked in both Ireland and the UK stated that he has had experiences “In both Ireland and the UK”. P2 spoke of a number of occasions in which he has had suspicions of substance use on site however with “alcohol only”.
Tom Browne (P4) has had a number of encounters with employees using illegal substances where he has had to “actually removed them from site.” P5 has had “some suspicions in [her] years of working as a health and safety officer”
The participants of the focus group gave similar opinions to the individual interviewees, FG1 believed that he “most definitely” suspected alcohol consumption on site, however, “I don’t believe I have seen any drugs on site.” FG2 agreed with FG1 highlighted that he has “smelt it off some guys a few times.” FG3 has had his suspicions but doesn’t believe you will see it on the site itself; “once on site I have seen it but I think you would see lads going off site to the pub or even drinking a can off-site in the back of their van more than you’d see it on the actual site.”
Of both the face-to-face interviews and the focus group only Tom Browne reported having had an accident on one of his sites in which alcohol was a contributory factor however, he would not go into too much detail on what exactly happened.
4.2.3 Link between accidents and alcohol/illicit drugs
All those interviewed were in agreeance that both alcohol and illicit drug use could be linked to accidents on site. One of the interviewees (P5) was of the opinion that although she believes there is a link, there are other factors that contribute to accidents more than alcohol or illicit drugs;
“Yes, I would think it does play a part but not as much as other factors such as carelessness, disrespect for rules, unawareness, poor supervision, poor training, rushing and stress.”
Tom Browne (P4) was in agreeance with P5 he believes that while alcohol and illicit drug use is linked to accidents on site it is not “exclusively” alcohol and illicit drugs that contribute to the accidents.
P2 believes that when it come to the use of alcohol the link is “not in present times but most definitely in the past.” However, he feels less strongly about a link between illicit drug use and accidents, stating that there is a possible link “but a fairly weak one.”
P1 highlighted that he had never seen an accident in which the root cause was alcohol in his 16-year career but believes that when you start to break down the accident it is definitely possible that it can be a factor;
“I never seen evidence of it thankfully, I hope I never do but when you look at an accident or an incident you start breaking it down you have to look at all possible causes there. So it is possible, yes, it could arise when you start looking at the root causes.”
While he has never witnessed the use of illicit drugs, P1 believes that alcohol use is more prevalent on site and as a result, it is more likely that a link between alcohol use and site accidents is prevalent;
“Never seen evidence of [illicit drug use] on site or in the canteens or drying rooms or wherever. I think you’d be more inclined to see possibly somebody having a few beers maybe or had a few beers the night before than drug use. Drug use is more hidden, more discrete.”
All three members of the focus group agreed with one another that they believe alcohol use and accidents on site are linked to each other with FG3 adding that “alcohol and drug toolbox talks have certainly convinced me that there is a link.” In terms of illicit drug use and accidents, all three believed they were linked however they had not experienced it in their careers. FG1 stated that he doesn’t know enough about today’s drugs but he would be worried of the effects it would have on certain members on the site;
“I don’t know enough about drugs today but I’d say it would definitely effect the lad up in the tower crane if he was off his head on something or the lads driving the diggers etc.”
4.2.4 Flaws in Safety, Health and Welfare at Work Act 2005
All interviewees were aware that there is no requirement for a worker to undergo testing for intoxicants under current health and safety legislation and that employers do not have a legal obligation to test their employees for intoxicants.
When asked if the Safety, Health and Welfare Act Section 13c was subject to abuse, Tom Browne (P4) stated that the employee is not abusing the clause, they are simply asserting their rights. He does however, believe that it needs to be improved.
“It is not so much abuse but rather the employee is simply asserting their right not to do so unless it is a condition of their employment contract therefore it needs to be tightened up.”
Like Tom Browne (P4), P2 believes that the situation needs to be improved by looking towards the labour rights legislation.
“I suppose the labour right legislation would need to be consulted in this instance as this is the reason that random testing is not permitted in Ireland.”
While P5 believes “it should be part of the contract”, P1 is “not sure if it’s even being pushed by any company. I don’t think it is even being enforced.”
Tom Sweeney (P3) believes that while employees aren’t legally obliged to take a test, they may still do so as to not want to look guilty;
“I have never been in a situation in Ireland where a drug or alcohol test has been considered. I don’t think that anyone would be willing to refuse a drug test without appearing guilty.”
Tom highlighted his experiences working in England in which he stated;
“In regard to Crossrail, I worked on the BAM Ferrovial Kier joint venture constructing the western running tunnels and SCL works. At induction, everyone completed a drug and alcohol test with an onsite nurse. There were about 3 or 4 failures at this stage during my 18 months on the project. Following that, we did 5-10% of the workforce weekly with the onsite nurse. The safety officer was responsible for the random selection as the nurse had to be seen to be independent. We had to document the process of making it ‘random’. On a failure, the site security escorted the individual from site. This required a lot of resources that I have not had on my Irish sites – nurses, security and a safety officer with a few hours to spare. A significant failing in this system is that the random tests were only for site personnel, and none of the management were tested. I know some of the management would have failed at certain times. In my personal selection of random drug and alcohol tests, I think I only had 2 failures, with 1 being from alcohol. In general, the system worked more as a deterrent than actually catching and kicking people off-site.”
The researcher asked those in the focus group how they would react to being asked to go and take a drug test and all stated that they would be open to it as it may one day save them should someone else on site become a hazard due to drug use;
“It was a big thing in England, to be tested every few weeks, I have never been tested here but I wouldn’t refuse having to be tested if they suspected me of being on something.” FG1
“I agree; I would not refuse it. They are looking out for the safety of the other workers and I want them to look out for me if they thought another man was drunk.” FG2
“Once they paid me!” FG3
4.2.5 Lack of drug testing conditions in contracts
Of the eight participants interviewed only two claimed to have drug testing incorporated into their contracts. Tom Browne (P4) stated having the drug testing condition in his employee’s contracts as did P2, the HSEQ manager of Company A. However, two health and safety officers with Company A denied having drug testing incorporated in their contacts with P5 simply saying “No” and P1 saying “no, as far as I know, it’s not. I’m with the company 16 years now.”
One of the participants of the focus group was unaware whether or not drug testing was incorporated into his contract.
4.2.6 Substance use course of action
As mentioned in 4.2.5, Tom Browne (P4) had drug testing incorporated into his employee’s contracts and therefore his course of action was to:
“subject them to a drug and alcohol test where refusal is a dismissible offence.”
Tom Sweeney (P3) revealed that his course of action would be to “simply remove or suspend the individual based on behavior. We have no system in place to conduct a drug or alcohol test based on suspicion.”
All three employees of Company A seemed to be on the same page when it comes to dealing with an individual on site possibly being under the influence or alcohol or another drug with all three consulting the individual’s employer first.
“We would have to consult with his employer and stand him down for his own and the safety of others.” P2
“Ensure they are OK and don’t require medical attention. As we deal with subcontractors mostly, we would look for their Employer to meet with us immediately. The Operative would most likely be dismissed from our site.” P5
“Firstly, don’t go head on in yourself. You have to deal with it in a certain sensitive way obviously, if they work for a sub-contractor, who we mostly have, it is important that the individual’s supervisor is advised that there is a suspicion that that individual may be intoxicated. You then agree a plan of how you’re going to deal with the situation. You obviously have to deal with it discretely and not a situation whereby the individual is made become embarrassed or posed as a threat to others. What you’d also ensure is that you have somebody there as a back-up. That you’re not dealing with the situation on your own. Only had one experience of this dealt with off-site. Follow it up logging it, report it internally in our own system just in case down the line that the guy took an unfair dismissal case so it’s important that it’s documented, where it happened, the time and the date and your reason behind it so you have to be careful. One of the things that we do it we would mention it drug and alcohol is part of our induction. Let the guys aware that we have procedures there.” P1
4.2.7 Workplace policies
All interviewees spoke of their company’s policy in relation to drugs and alcohol with each giving slightly different responses. P1 mentioned that Company A have various policies that make up a company handbook and that that handbook is distributed to sub-contractors on their site.
Intoxicants on Company A sites are “a definite no-no, we have a policy in the company. It is there. A lot of our employees would be sub-contractors so as a company we would have our own policies that forms part of our company safety statement and our employee’s handbook but it would be interesting to see if other companies go to that level. It is probably something worth investigating to see if your small, medium or large sized companies do have good robust policies and if they’re being followed through.”
P5, also with company A added that “persons taking medications for health reasons should declare this to us at Induction and we would ensure that that medication doesn’t impact on their ability to work safely.” P2, HSEQ manager of Company A further added that intoxicants are “not permitted and are covered in the induction. It is also part of our disciplinary procedure.”
Tom Browne (P4) spoke of how his policy offered the individual some assistance once they co-operate;
“…where an employee divulges to the company that they have a problem with substance/alcohol abuse they are afforded Employee Assistance whereby their recovery is assisted but they must cooperate.”
Tom Sweeney (P3) simply stated that his company’s policy is “as per the SHWW 2005, an individual is not allowed to be under the influence of any intoxicants.”
4.2.8 Future Problems
There was a quite mixed reaction when interviewees were asked of a potential increase in alcohol and/or drug use on Irish construction sites in the next number of years with more jobs becoming available accompanied with a potential rise in wages.
P1 sees a possible link between increased wages and the use of alcohol and drugs on site especially with the younger cohort coming in;
“I suppose it could because people are going to have more disposable income and that often leads to people trying to get another high as such, so it’s very likely for younger people coming in and they’re going to start earning good money, that would be a core group I would see where it could be an issue. It could be open to abuse of drugs etc.”
P2 very much agrees with his colleague stating that “particularly in the young male cohort as these guys will have plenty of disposable income and no real responsibilities.”
The participants of the focus group agreed amongst one another of the potential increase in drug/alcohol use in the future;
“it is possible, if people have more money they have more money to spend on things like that.” FG1
“I agree with P1” FG2
“Yes, especially with the young lads coming in.” FG3
Tom Sweeney (P3) believes that it will be as much a problem in the future as it is now;
“No more of an issue than it is now. As labour becomes scarce, then perhaps people who are less able to manage work with their drug or alcohol problems will re-enter the workforce.”
However, both Tom Browne (P4) and P5 tend to disagree that money and a young workforce has the potential to cause a rise in alcohol and drug use on Irish construction sites;
“I don’t see the problem as wage related as addiction is not driven by disposable income.” Tom Browne (P4)
“No, if anything I would expect it to me more a problem in recession times where people may abuse substances to cope with difficult times.” P5
4.2.9 Introduction of random drug testing in Ireland
All participants felt strongly about the introduction of random drug testing in Ireland with P1 seeing it being introduced in the next few years. He believes there is work to be done in order to get it passed such as getting the relevant bodies on board and having suitable data to back it up;
“Yes, I would definitely agree with that. I think if anything that if it’s up and running in the UK and it’s working well and it’s showing a positive outcome that it probably will eventually come in here. It’s probably something that will come in in the next 4/5 years. I think what will happen first is the relevant bodies, the Garda, the HSA, the Unions would have to be involved, different work groups IVEC and so forth would be there as well, so you’d have to make sure that you have a good firewall in place there before you would tackle it. So there is a lot of interested bodies there and you need to ensure that you’re showing the reasons behind it and why you’re doing it. The other thing is that it’s very good to have some form of research there to back it up rather than just going at it. If you’ve got good data there to back it up, it makes it a lot easier to bring it in and make it work.”
Tom Sweeney (P3) added that he “worked on a project in the UK that has drug and alcohol testing at induction, and then randomly afterwards. I think this was a good thing, and I would like to see it in use in Ireland.”
Tom Browne (P4) simply believes that if an individual is refusing to sign the random drug testing condition, the employer should not employ them;
“it is Law in Ireland but there are difficulties with widespread implementation however each employer may transpose this into their Safety Statement and induct this to their workforce and have them sign it. The employer should not employ a person refusing to sign up to this condition.”
4.3 Analysis
Under this heading, findings will be discussed in relation to the relevant literature. It will discuss the emerging themes from both methodologies. This heading will be presented under the following sub-headings:
- Prevalence of alcohol and drug use in the construction industry in Ireland;
- Substance abuse related-workplace accidents;
- Employer and Employees duties regarding alcohol and illicit drug use in construction;
- Remedies and actions that may combat substance abuse.
4.3.1 Prevalence of alcohol and drug use in the construction industry
The data collected from the primary research and secondary research revealed quite a bit of information regarding substance abuse on Irish construction sites. The secondary research data revealed information about substance use in Ireland as a whole. However, there was not much information available regarding substance abuse in the construction industry in Ireland alone. Although, data was obtained regarding substance abuse in the construction industry in the United Kingdom and United States of America etc. By taking the growing substance abuse population in Ireland as a country and implementing this into the general rate of those abusing substances into the construction industry in the UK and USA, the researcher was able to develop a fair idea of the prevalence of substance abuse in the Irish construction industry. The NACDA survey of drug prevalence in Ireland revealed a continuous increase in the prevalence of drug use in the country through the four surveys conducted between 2002 and 2015. It was also revealed in the literature review through the Healthy Ireland Survey (Department of Health, 2016) that 55% of drinkers, drink at least once a week, with those aged 55-64 drinking the highest weekly (66%) with a significant difference between male and female, 68% and 52% respectively. Considering the construction industry is dominated by a male workforce it could be considered that a number of these men are working within the industry in some form. The Alberta Alcohol and Drug Use Commission (AADAC) (2002) prevalence survey found that the construction industry was regarded as a group of concern in terms of rates of substance use.
Larson, et al (2007) found that full-time American construction workers aged 18-64, had the highest rate of past month alcohol use compared to workers in all other industries at 16%. As previously stated, Rountree (An assessment of drug testing in the construction industry, 2002) found that there was almost double the amount of heavy alcohol users among construction workers (12.4%) than the national average for other industries (7.6%).
Hogan, et al (Construction apprentices’ attitudes to workplace drug testing in Ireland, 2006) survey highlighted that 4.6% of the Irish construction apprentices that were surveyed reported having an accident due to the use of alcohol while 3.6% reported to having an accident due to drug use. Applying those percentages to the total number of apprentices in the country (15,614 – construction apprentices) and if 4% of apprentices reported an accident due to the use of alcohol or other drugs, 625 people would suffer an accident in a year with alcohol or drug use contributing to the accident.
Through the primary research, the researcher received quite a mixed reaction from those interviewed. It is clear that the Irish construction industry has certainly witnessed substance abuse at some point with certain interviewees mentioning that substance abuse on construction sites in Ireland being a thing of the past while others such as Tom Sweeney believes it is still an on-going situation. This can be backed up by the anonymous labourer from the London site who claimed to have witnessed drug dealing on site for months with management completely aware; “There is one particular site in London where a lad has been dealing drugs for months. It’s not really done underhand; everybody knows he’s the man to contact to score drugs, and he knows he has a large marketplace to make money.”
Each interviewee spoke of their own suspicions of workers on their sites being under the influence. One interviewee in particular revealed an experience of his own in which an employee was seen consuming alcohol and was subsequently dealt with off-site while another had an employee he had to remove from site for using a form of drug whilst at work. Tom Sweeney highlighted that he had witnessed alcohol and drug use on Irish construction sites.
All of the interviewees showed their belief in the link between substance abuse and workplace accidents. Whilst some believed it was a definite contributory factor, others believed it was just as much a factor as poor training or carelessness etc.
Through the focus group, it was found that the three interviewees were concerned about what could potentially happen to them should someone else on site be under the influence of an intoxicant possibly knowing that they cannot be randomly selected for testing. These results were similar to take of construction workers in the UK. Of the 1300 construction workers surveyed, 59% had concerns over the effects of drugs and alcohol on site while 39% stating the issue of drugs and alcohol could be better tackled and 35% noticing a co-worker under the influence.
Through research conducted in similar working conditions to that of the construction industry such as manufacturing plants etc. the majority of researchers found reason to believe that alcohol and drug use is a contributory factor to workplace accidents. Mangione, et al (Employee drinking practices and work performance, 1999) found that there was a relationship between alcohol use and injuries with heavy drinkers having the highest rate while Shipp, et al (Substance use and occupational injuries among high school students in South Texas, 2005) found that risk of injury increased for all substances with higher rates of current and lifetime use.
From the findings from the literature review and the qualitative data it can be seen that substance abuse is somewhat prevalent in the Irish construction industry but not at a monumental scale. It also showed that the taking of substances can have some very negative effects on how an individual reacts to their work and the hazards they pose as a result.
4.3.2 Substance abuse-related workplace accidents
The researcher reviewed literature with the aim of investigating the relationship between substance use and misuse and occupational injuries. The researcher found through Stallones & Kraus (The Occurrence and Epidemiologic Features of Alcohol Related Occupational Injuries, 1993) that there was not enough evidence available to establish a relationship between alcohol use and misuse and workplace injuries. However, the IOM’s conducted a more detailed review of the impact of alcohol and other drugs in the workplace and their outcomes including job satisfaction, absenteeism and accidents. Through this report, the researcher learned that while there was evidence that substance abuse effected job behaviour and occupational outcomes including injury negatively, substance use’s influence on these injuries were small. The study showed that there is a lack of analytical approaches to the study limiting their ability to say anything definite about a drug/accident relationship. Most available studies lacked controls for personality traits and other risk taking dispositions in multivariate models.
The researcher looked at a number of different studies which found wide, positive effects on self-reported alcohol use on occupational injuries. The researcher found through Stallones & Xiang (Alcohol consumption patterns and work related injuries among Colorado farm residents, 2003) that the consumption of alcohol had a large effect on reporting a work-related injury. Those who drank alcohol three or more on average, had about 3.2 injuries per 10,000 person-work-days (c. 40-years’ work) compared to 1.9 injuries per 10,000 for those who do not drink alcohol, a 70% increase in risk. 3.2 injuries per 10,000 person-work-days is a yearly rate of 8 injuries per 100 workers. If 10 million workers are drinkers (from 140 million) there would be over 320,000 yearly injuries due to alcohol. The researcher then learned that a positive relationship between drinking five or more drinks daily in the past twelve months and having a workplace injury among respondents in the 1998 National Health Interview Survey.
Through the interviews, the researcher found that those interviewed agreed that both alcohol and illicit drug use could be linked to accidents on site. P1 believed that when you start to break down the accident it is definitely possible that it can be a factor. He also stated that alcohol use is more prevalent on site and as a result, it is more likely that a link between alcohol use and site accidents is prevalent. It can be found that there are factors that can contribute more to accidents on site such a poor training or simply a disrespect for rules like P5 mentioned in her interview.
From the findings from the literature review and the qualitative data it can be seen that alcohol and illicit drug use can be a contributory factor towards accidents occurring on site however in present day it is not one of the main contributory factors on construction sites in Ireland.
4.3.3 Employer and Employees duties regarding alcohol and illicit drug use in construction
The literature review revealed that there is no requirement for a worker to undergo testing for intoxicants under current health and safety legislation. Likewise, employers do not have a legal obligation to test their employees for intoxicants. The relevant duties of the employer are set out in Section 8 of the Act (Health and Safety Authority, 2005). These duties require the employer to ensure, so far as reasonably practical, the safety, health and welfare of all his or her employees.
The employee must ensure that they are not under the influence of an intoxicant that may result in them endangering themselves or other people present at the time, Section 13(1)(b). The employee must also fully co-operate with their employer to comply with health and safety law e.g. an employer should inform their employer if they are taking any medication that may pose a risk to other workers.
It can be seen from the research findings that all interviewees believed there was a need for a stricter way of dealing with the potential substance abusers on site. While all interviewees revealed they had policies regarding alcohol and drugs, not all of them had drug testing incorporated into their employee’s contracts meaning employees could simply refuse to take a drug test if they are suspected of being intoxicated in some form. Those interviewed who had previously worked in countries in which random drug testing was carried out were strongly in favour of introducing it here after they saw the positive outcome it had. Considering some of the companies a number of the interviewees are employed to have no drug testing condition, individuals could use substances and get away with it as they are not required to take a drug test. Tom Sweeney mentioned that he only witnessed two failures and that the system is more of a deterrent than a way of catching people out. Therefore, workers in the UK etc. may not be willing to take such a risk as they never know when they will be sent to be tested.
All interviewees agreed with one another that random drug testing should be introduced in Ireland with one believing we will see it in the next 5 years.
From the findings from the literature review and the qualitative data it can be seen that while the employer is not legally obliged to test his/her employees, they must provide a duty of care towards them. The employer must ensure, so far as reasonably practical, the safety, health and welfare of all his or her employees. They therefore must manage and conduct work activities to prevent improper conduct or behaviour that will likely put employees at risk. As for the employee, the researcher learned that they must ensure that they are not under the influence of an intoxicant in which they could endanger themselves or the other people present at the time. The employee must fully co-operate with their employer to comply with health and safety law. The researcher found that employers should address whether the employee’s behaviour poses a risk of danger to himself/herself or others and remove them from site if necessary.
The researcher found through the interviews that only two of the eight interviewees claimed to have drug testing incorporated into their contracts. Tom Browne (P4) claimed to having the drug testing condition in his employee’s contracts. P2, the HSEQ manager of Company A also claimed this condition in his employee’s contracts, however, two health and safety officers with the same denied this.As an employer, Tom Browne (P4) believed his duty toward an offender would be to subject the party to a drug test in which refusal to do so would be a dismissible offense due to the condition clearly stated in the employee’s contract
The researcher found that in a case where an individual was under the influence of an intoxicant it would be done in a professional way in which the individual’s employer would be notified and the situation would be sorted so as not to embarrass the individual. Tom Browne also spoke of seeking help for the individual on the condition that they fully co-operated.
4.3.4 Remedies and actions that may combat substance abuse
Through the literature review and various interviews, the researcher found that there were numerous ways to try and combat substance abuse on construction sites. The researcher learned that by identifying substance abuse early can save employers and companies money in terms of health and productivity costs. An employer can set up a substance abuse programme that includes workplace policies, drug testing, employee educational promotion, employee assistance programmes (EAP’s) and health plan treatment coverage. The programme would include confidential screening by an EAP or health professional, an education component, treatment referrals to an EAP or health professional as well as confidential follow up care for supporting any employees in recovery.
The researcher discovered that by creating a substance abuse policy a drug-free workplace is more likely. Some industries have specific legal obligations to address workplace substance abuse. Employers may offer their employees access to an Employee Assistance Programme (EAP). The EAP provide information, referrals and counselling on issues such as substance use, stress, family problems, mental health and work. The EAPs guide employers in addressing various employee problems and proactively deal with workplace issues that may lead to violence, declining morale and physical and mental health issues. The programmes are staffed by professionals who provide the individuals and their families with prevention services and short term problem-resolution services.
The researcher found that health plans would be another ideal way to combat substance abuse on site. It would provide coverage for substance abuse screening, therapy, counselling and aftercare. By offering a comprehensive health plan with benefits, employers can help make treatment successful. An employer can play a major role in preventing the hazardous use of legal and illegal substances by making it clear that drinking and the use of illicit drugs on site is not condoned, that employees can get treatment confidentially without jeopardizing their jobs while being educated about drugs and alcohol.
Sisk have a Substance Abuse policy which they implement across all their jobs in the UK. As part of the induction to site, employees were informed company’s Substance Abuse policy and informed them that random drug and alcohol testing would be carried out every six weeks during the project. Toolbox talks were also given throughout the course of the project.
Ballymore put together a series of health and safety awareness features. The implementation of on-site testing and easily accessible support systems shows that the company is committed to a direct action approach to the situation. Guidance and support systems were offered to individuals who admitted their drug or alcohol problem before being testing, encouraging an attitude of seeking help. Ballymore’s drug and alcohol toolbox talks were constructed with a designed approach to educate the workforce on the important information on drug and alcohol use. FRANK is a contact source for drug support and advice service. A site phone was provided for anyone who did not feel comfortable expressing themselves to the site’s own advisors. The researcher also found that Ballymore used the “Here’s my reason. What is yours?” campaign to combat drug use on site. The posters portrayed why it’s important to stay alert and maintain safety, with a thoughtful reason in mind.
In the interviews participants felt strongly about the introduction of random drug testing in Ireland with P1 believing it will be introduced in the next few years.
Chapter 5: Conclusion and Recommendations
5.1 Aim and Objectives
Firstly, a discussion on whether the overall aims and objectives of the thesis were achieved. This study was completed within the designated time frame. Given the allocated time frame and resources that were available to complete the thesis, the researcher is satisfied that the overall aim and objectives of the study have been achieved.
5.1.1 Aim of research
The aim of the dissertation was to investigate and examine substance abuse and its presence in the Irish Construction Industry.
5.1.2 Research Objectives
- Investigate drug abuse in Ireland and the Construction Industry.
- Examine the substances most commonly associated with workplace related accidents.
- Detail the Employer’s position and legal duties in relation to substance abuse on Irish construction sites.
- Investigate and propose possible remedies/actions that can be taken to combat substance abuse on construction sites in Ireland.
5.2 Achievement of aim and objectives
Overall the researcher of this thesis feels that the aims and objectives set at the beginning of the study have been achieved. The study has identified the prevalence of substance abuse in the construction industry in Ireland. The research has also established the consequences of what may happen on site as a result of drug use as well as the employer’s duties and how substance abuse may be combated.
It confirmed through interviews and a literature review that while it can be said that substance abuse is a thing of the past, many people still believe it exists today and in some cases management are turning a blind eye to it for reasons such as to not affect morale.
The various case studies showed first-hand what happens on a construction site when workers are in fact taking some form of drug.
The overall study has highlighted that there is not sufficient published data available in relation to substance abuse in the Irish construction industry itself. Instead the researcher chose to firstly look at drug use in Ireland and then to look at the worldwide construction industry in a bid to look into the mind-set of a construction worker. In doing it this way, the researcher found that there has been a rise in the use in illicit drug use in young Irish adults and that Irish adults drank more dangerously than any other country. The researcher also found that in America, illicit drug and alcohol abuse and dependence was nearly twice as prevalent in the construction industry than any other industry. The majority of those interviewed stated that it was either once a problem or even still is. From information such as this, the researcher was able to determine that substance abuse certainly exists in the Irish construction industry but is not necessarily prevalent.
5.3 Limitations during the Research
The researcher believes that the research targets were both realistic and achievable. However, gathering data on the prevalence of substance abuse on construction sites in Ireland alone proved difficult as there is not a lot of literature on it nor have the Health and Safety Authority published any figures regarding accidents as a result of drug use etc. However, the researcher believes that the way in which the thesis was broken down formed a good base of this research that tested the hypothesis.
5.4 Recommendations
The researcher believes that the question set out at the beginning of the research has been supported throughout the course of the study. However, the researcher believes that more research needs to be conducted through statistics etc. by the Health and Safety Authority and various other bodies such as the Construction Industry Federation to determine exactly how prevalent substance abuse is on Irish construction sites. The researcher hopes that the prevalence that exists today will be rectified within the coming years through the introduction of random drug testing which certainly seems to be working in other countries.
References
Alberta Alcohol and Drug Abuse Commission. (2002). Substance use and gambling in the Alberta workplace. Edmonton, Alberta: Alberta Alcohol and Drug Abuse Commission.
Alvania, S., Berg, T. v., & Duivenbooden, C. v. (2009). Impact of work-related factors, lifestyle and work ability on sickness absense among Dutch construction workers. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/19554244
American Psychiatric Association. (2000). Practical guidelines for the treatment of psychiatric disorders (1 ed.). Washington D.C.: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Health Disorders (5th Edition ed.). Washington D.C., USA: American Psychiatric Association.
Ames, & James. (1990). The Changing Workplace, Alcohol Problems & Well-Being (8th Edition ed.). Colorado: McGraw-Hill.
Ames, G., Grube, J., & Moore, R. (1997). The relationship of drinking and hangovers to workplace problems (1st Edition ed.). Berkely, California, USA: Unknown.
Bass, A., Reid, R. B., Delaphane-Harris, K., Schork, M., Kaufmann, R., McCann, D., . . . Cook, S. (1996). Employee drug use, demographic characteristics, work reactions and absenteeism. Occupational Health Psychology, 1(1), 92-99.
Blume, S. (1998). Alcohol and Drug Abuse in the Encyclopedia of Occupationsla Health and Safety (4th ed.). Geneva: International Labour Office.
Bowling, A. (2014). Research Methods in Health. Buckingham: Open University Press.
Broughton, T. (2001). The drug problem. Retrieved from http://www.building.co.uk/the-drug-problem/1008996.article
Bryman, A., & Bell, E. (2011). Ethics in Business Research. Retrieved March 30, 2017, from https://intranet.mbs.ac.uk/Portals/0/docs/Ethics/Bryman%20Bell%20(2007)%20Ethics%20in%20business%20research.pdf
Canadian Centre for Occupational Health and Safety. (2005). Substance Abuse in the Workplace. Retrieved March 19, 2017, from http://www.ccohs.ca/oshanswers/psychological/substance.html
Considerate Constructors Scheme. (2016). Case Study: Ballymore. Retrieved April 2, 2017, from https://ccsbestpractice.org.uk/wp-content/uploads/2016/06/Ballymore-Group1.pdf
Considerate Constructors Scheme. (2016). CASE STUDY: John Sisk & Son Ltd. Retrieved April 2, 2017, from https://ccsbestpractice.org.uk/wp-content/uploads/2016/06/Sisk1.pdf
Considerate Constructors Scheme. (2016). Case Study: Mulalley and Co Ltd. Retrieved April 2, 2017, from https://ccsbestpractice.org.uk/wp-content/uploads/2016/06/Mulalley1.pdf
Construction Industry Federation. (2003). Compliance of Workers. Retrieved March 15, 2017, from http://csponline.ie/wp-content/uploads/2014/08/JSC_leafletComplianceofWorkers.pdf
Cook, R., Hersch, R., Back, A., & McPherson, T. (2010). The Prevention of Substance Abuse among Construction Workers: A Field Test of Social-Cognitive Programme. Primary Prevention, 25(3), 337-357.
Cunradi, C., Todd, M., M, D., & Ames, G. (2009). Problem Drinking, Unemployment, and Intimate Partner Violence among a Sample of Construction Industry Workers and their Partners. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217036/
Dawson, D. (1994). Heavy drinking and the risk of occupational injury. Accident analysis and prevention, 26(5), 655-665.
Department of Health. (2012). Steering Group Report on Substance Misuse Strategy. Retrieved from http://www.drugsandalcohol.ie/16908/2/Steering_Group_Report_on_a_National_Substance_Misuse_Strategy_-_7_Feb_11.pdf
Department of Health. (2016). The Healthy Ireland Survey. Dublin: The Stationary Office.
Department of Health and Children. (2002). Strategic Task Force on Alcohol. Dublin: Government Publications.
Designing Buildings. (2017). Construction Plant. Retrieved from https://www.designingbuildings.co.uk/wiki/Construction_plant
EAP Institute. (-). Drugs and Alcohol at Work. Retrieved March 15, 2017, from http://eapinstitute.com/documents/EAP_Institute_DrugTesting.pdf
Eastern Regional Health Authority. (1997). Developing policy on alcohol, tobacco and drug use (1st ed.). Dublin: Eastern Regional Health Authority.
Employee Assistance Professionals Association. (2017). What is an EAP. Retrieved March 20, 2017, from https://eapaireland.ie/what-is-an-eap/
European Commission. (2010). EU citizens’ attitudes towards alcohol. Retrieved from http://ec.europa.eu/public_opinion/archives/ebs/ebs_331_en.pdf
European Monitoring Centre for Drugs and Drug Addiction. (2003). The state of the drugs problem in the European Union and Norway. Lisbon: European Monitoring Centre for Drugs and Drug Addiction.
Frone, M. (1998). Predictors of work injuries among employed adolescents. Applied psychology, 83(4), 565-576.
Gemmell, C., Moran, R., Crowley, J., & Courtney, R. (1999). Literature Review on the Relation between Drug Use, Impaired Driving and Traffic Accidents. Retrieved from http://www.drugsandalcohol.ie/11649/1/EMCDDA_Lit_review_drug_use_impaired_driving.pdf
Government of South Australia. (2006). Guidelines for addressing alcohol and other drugs in the workplace. Adelaide: Governemnt of South Australia.
Harrison, T. S. (1950). Harrison’s Principle of Internal Medicine (19th Edition ed.). Birmingham, Alabama, USA: McGraw-Hill.
Hawkes Group. (2016). Hawkes Group Drug and Alcohol Policy. Retrieved from http://hawkesgroup.co.uk/wp-content/themes/hawkes/downloads/drugs-alcohol-policy.pdf
Health and Safety Authority. (2005). Health, Safety and Welfare at Work Act 2005. In HSA (Ed.), Health, Safety and Welfare at Work Act 2005 (p. Section 13 (1)(c)). Dublin, Ireland: HSA.
Health and Safety Authority. (2005). Safety, Health and Welfare at Work Act 2005, Section 19. Retrieved March 14, 2017, from http://www.irishstatutebook.ie/eli/2005/act/10/enacted/en/print#sec19
Health and Safety Authority. (2005). Safety, Health and Welfare at Work Act 2005, Section 20. Retrieved March 14, 2017, from http://www.irishstatutebook.ie/eli/2005/act/10/enacted/en/print#sec20
Health and Safety Authority. (2005). Safety, Health and Welfare at Work Act 2005, Section 8. Retrieved March 14, 2017, from http://www.irishstatutebook.ie/eli/2005/act/10/enacted/en/print#sec8
HJ Lipscomb, J. D., & Li, L. (2003). Health care utilisation of carpenters wuth substance abuse-related diagnoses. American Journal of Industrial Medicine, 120-131.
Hoffman, J., & Larison, C. (1999). Drug use, workplace accidents and employee turnover. Drug use, 29(2), 341-364.
Hogan, V., Cannon, R., & Gabhainn, S. N. (2006). Construction apprentices’ attitudes to workplace drug testing in Ireland. National University of Ireland Galway. Galway: Ingenta.
Horgan, C., Skwara, K., & Strickler, G. (2001). Substance Abuse: The National Number One Health Problem (1st ed.). Waltham: Bardeis University.
Human Resources Council. (2017). Workplaces that Work. Retrieved March 20, 2017, from http://hrcouncil.ca/hr-toolkit/workplaces-health-safety.cfm
Iacuone, D. (2005). Real men are tough guys. Retrieved from http://eds.b.ebscohost.com/eds/pdfviewer/pdfviewer?sid=40dc7f98-e638-4c1d-800a-6ae0b5641784%40sessionmgr103&vid=2&hid=104
International Labour Organisation. (2003). Drug and Alcohol Abuse Prevention. Geneva: International Labour Organisation.
Irish Statute Book. (2004). Equality Act 2004. Irish Statute Book, 1(1), Varies.
James Boyle v Portalan trading as Wagamama, UD1735/2014 (January 25, 2016).
Kaestner, R., & Grossman, M. (1998). The Effect of Drug Use on Workplace Accidents. Labour Economics, 5(3), 267-294.
Krueger, R. A. (2015). A Practical Guide for Applied Research. Minnesota: SAGE.
Laad, P., Chaturvedi, B. A., & Shaikh, M. (2013). Prevalence of substance abuse among construction workers. Prevalence of substance abuse among construction workers, 2(3), 281-282.
Larson, S., Eyerman, J., Foster, M., & Froeter, J. (2007). Worker Substance Use and Workplace Policies and Programs. Department of Health and Human Services. Rockville: Department of Health and Human Services.
Lehman, W., & Simpson, D. (1990). Employee substance abuse and on-the-job behaviours. Applied Psychology, 77(3), 309-321.
Manaf, Z. B., & Najib Razali, M. (2007). THE MANAGEMENT OF PLANT AND MACHINERY AT CONSTRUCTION SITE: IT’S IMPACT ON THE COMPLETION TIME OF CONSTRUCTION PROJECTS. Kuala Lumpur: Management in Construction Researchers Association.
Mangione, T., Howland, J., Amick, B., Cote, J., Lee, M., Bell, N., & Levine, S. (1999). Employee drinking practices and work performance. Studies of Alcohol, 60(2), 261-270.
Mark, T., Coffey, R., & King, E. (2000). Spending on mental health and substance abuse treatment, 1987-1997. Spending on mental health and substance abuse treatment, 1987-1997, 19(1), 108-120.
Martin, J., Barry, J., Goggin, D., Morgan, K., Ward, M., & O’Sulleabhain, T. (2010). Alcohol-Attributed mortality in Ireland. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/20530495
McLellan, A., Lewis, D., O’Brien, C., & Kleber, H. (2000). Implications for treatment, insurance and outcomes evaluation. Drug Dependence, a Chronic Medical Illness, 284(13), 1689-1695.
Morgan, K., McGee, H., Dicker, P., Brugha, R., Ward, M., & Shelley, E. (2009). Survey of lifestyle, attitudes and nutrition in Ireland. Dublin: Department of Health and Children.
Naoum, S. (2007). Dissertation Research & Writing for Construction Students (2nd ed.). Oxford: Elsevier.
National Advisory Committee on Drugs and Alcohol. (2015). Prevalence of Drug Use and Gambling Ireland and Drug Use in Northern Ireland 2014/15. Retrieved from http://nacda.ie/images/stories/docs/publicationa/nacda-bulleti-2-prevalence-drugusegambling-rdatfhsct.pdf
National Business Group on Health. (2009). An Emplyer’s Guide To Workplace Substance Abuse. Retrieved March 15, 2017, from http://www.workplacementalhealth.org/Business-Case/An-Employers-Guide-to-Workplace-Substance-Abuse-Strategies-and-Treatment-Recommendations-.aspx?FT=.pdf
National Center for Biotechnology Information. (2017). Screening and Assessment. Retrieved March 20, 2017, from http://hrcouncil.ca/hr-toolkit/workplaces-health-safety.cfm
National Institute of Health. (2001). Alcoholism: Getting the facts. Bethesda: National Institute on Alcohol Abuse and Alcoholism.
National Institute on Alcohol Abuse and Alcoholism. (2011). Alcohol Use and Preventing Alcohol-Related Problems Among Young Adults in the Military. Retrieved March 6, 2017, from https://pubs.niaaa.nih.gov/publications/arh284/252-257.htm
Normand, J., Lempert, R., & O’Brien, C. (1994). Under the influence? Drugs and the American workforce (3rd ed.). Washington D.C.: National Academic Press.
Normand, J., Salyards, S., & Mahoney, J. (1996). An evaluation of pre-employment drug testing. Occupational Health Psychology, 75(6), 629-639.
O’Connell, H., Lawlor, B., & Cunningham, C. (2004). A systematic review of the utility of self-report alcohol screening instruments in the elderly. A systematic review of the utility of self-report alcohol screening instruments in the elderly, 19(11), 1074-1086.
O’Connor, J., & Keenaghan, C. (1993). Alcohol and drugs in the workplace; attitiudes, policies and programmes in Ireland (1st Edition ed.). Dublin: Internation Labour Organisation.
OECD. (2011). Health Status. Retrieved from http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT
Oppenheim, A. (2000). Questiobbaire design, interviewing and attitude measurement. London: Continuum.
Paul Melia. (2006). Tram driver sacked for failing surprise breath test. Dublin: The Independent.
Prichard, D. R. (2000, October 25). irmi.com. Retrieved March 10, 2017, from https://www.irmi.com/articles/expert-commentary/substance-abuse
Princeton, N., & Wood, R. (2001). Substance Abuse, The Nation’s Number One Health Problem (1st Edition ed.). Waltham: Brandies University.
Quinlan, M. (2008). Corporate Training. Retrieved March 15, 2017, from http://www.corporatetraining.ie/drugs-and-alcohol-at-work.html
Ragland, D., Krause, N., & Greiner, B. (2002). Alcohol consumption and incidence of workers’ compensation claim. Alcoholism: Clinical and Experimental Research, 26(1), 1388-1394.
Rajasekar, S., Philominathan, P., & Chinnathambi, V. (2013). Research Methodology. Retrieved March 27, 2017, from https://arxiv.org/pdf/physics/0601009.pdf
Rassool, G. H. (1998). Substance Use and Misuse: Nature, Context and Clinical Interventions (1st Edition ed.). London, UK: Wiley Blackwell.
Rountree, P. (2002). An assessment of drug testing in the construction industry. Retrieved from https://www.aiha.org/aihce04/handouts/rt227rountree1.pdf
Royal College of Psychiatrists. (1987). Drug and Alcohol Review. London: Royal College of Psychiatrists.
Safety & Health Practitioner. (2016). Alcohol and drugs in UK construction industry placed under spotlight. Retrieved March 30, 2017, from http://www.shponline.co.uk/alcohol-and-drugs-in-uk-construction-industry-placed-under-spotlight/
Shipp, E., Tortolero, S., Cooper, S., Baumler, E., & Weller, N. (2005). Substance use and occupational injuries among high school students in South Texas. Drug and Alcohol abuse, 31(2), 253-265.
Smith, D. (2008). Tobacco smoking by occupation in Australia and the United States. 77-89.
Sonnenstuhl, W. J., & Trice, H. M. (1990). Strategies For Employer Assistance Programs (1st Edition ed.). Ithaca, NY, USA: ILR Press.
Stallones, L., & Kraus, J. (1993). The Occurrence and Epidemiologic Features of Alcohol Related Occupational Injuries. Addiction, 88(7), 945-951.
Stallones, L., & Xiang, H. (2003). Alcohol consumption patterns and work related injuries among Colorado farm residents. Preventive Medicine, 25(1), 25-30.
U.S. Department of Health & Human Services. (2002). National Evaluation Data Services (1 ed.). Rockville: Substance Abuse and Mental Health Services Administration.
U.S. Department of Health & Human Services, Centers for Disease Control and Prevention. (-). Alcohol problems among emergency department patients. Retrieved March 19, 2017, from https://www.cdc.gov/ncipc/pub-res/alcohol_proceedings/alcohol_proceedings
U.S. Department of Health & Human Services, Substance Abuse and Mental Health Administration. (2007). Drugs in the workplace: what an employer needs to know. Retrieved March 19, 2017, from http://workplace.samhsa.gov/DrugTesting/Files_Drug_Testing/FactSheet/factsheet041906.aspx
U.S. Department of Health & Human Services, Substance Abuse and Mental Health Services Administration. (2009). 14 short employer cost savings briefs. Retrieved March 19, 2017, from https://workplacepossibilities.com/wp-content/uploads/BNA-Drugs-and-the-Workplace.pdf
U.S. Department of Health and Human Services. (2007). National Expenditures for Mental Health Services and Substance Abuse Treatments 1993-2003. Rockville: Substance Abuse and Mental Health Administration.
U.S. Department of Health and Human Services. (2007). Understanding drug abuse and addiction. Retrieved March 19, 2017, from http://www.nida.nih.gov/Infofacts/understand.html
Veazie, M., & Smith, G. (2000). Heavy drinking, alcohol dependence and injuries at work among young workers in the United States labour force. Alcoholism: Clinical and Experimental research, 24(12), 1811-1819.
Wells, S., & MacDonald, S. (1999). The relationship between alcohol consumption patterns and car, work, sports and home accidents for different age groups. Accident Analysis and Prevention, 31(1), 21-27.
World Health Organisation. (2009). Evidence for the effectiveness and cost-effectiveness of intervention to reduce alcohol related harm. Copenhagen: World Health Organisation.
World Health Organisation. (2013). World Health Organisation. Retrieved February 27, 2017, from http://www.who.int/topics/substance_abuse/en/
World Health Organisation. (2014). The Global Status Report on Alcohol. Geneva: World Health Organisation.
Yin, R. K. (2014). Case Study Research; Design and Methods. Pennsylvania: SAGE.
Zikmund, W. (2013). Business Research Methods (9th Edition ed.). Mason: Erin Joyner.
Interview Questions
- Do you believe that substance abuse is prevalent on construction sites in Ireland at present or even in the past?
- Have you ever suspected a worker using illicit drugs or consuming alcohol during working hours on a construction site?
- Have you ever had an incident occur on site in which one of the factors turned out to be the intoxication of a site employee?
- A study carried out by the U.S. Department of Labour found that both illicit drug abuse & dependence and alcohol abuse & dependence was nearly twice as prevalent in the construction industry (average) than it was in all other industries, does this surprise you?
- From your experience do you believe that there is a possible link between alcohol use and workplace accidents?
- From your experience do you believe that there is a possible link between illicit drug use and workplace accidents?
- What is your take on Safety, Health and Welfare at Work Act 2005 Section 13c? Is it subject to abuse i.e. employees refusing to take a drug test if not in their contract?
- Is drug testing incorporated into your employee’s contracts?
- What would the course of action be on your site if you believed a worker was intoxicated and posed a threat to others?
- What are your workplace policies regarding intoxicants?
- With the industry recovering and wages potentially rising, can you see drug use possibly becoming an issue in the future?
- Should it be health and safety law that employers can send employees for random testing for intoxicants like in the UK?
Cite This Work
To export a reference to this article please select a referencing stye below:
Related Services
View all


Related Content
All TagsContent relating to: "Health and Social Care"
Health and Social Care is the term used to describe care given to vulnerable people and those with medical conditions or suffering from ill health. Health and Social Care can be provided within the community, hospitals, and other related settings such as health centres.
Related Articles

DMCA / Removal Request
If you are the original writer of this dissertation and no longer wish to have your work published on the UKDiss.com website then please: